Vous aimerez peut-être aussi
- Lactose Sources and Intolerance TypesDocument5 pagesLactose Sources and Intolerance TypesAngelica IsabelPas encore d'évaluation
- Lactose Intolerance: Presented by B1 Group 2Document27 pagesLactose Intolerance: Presented by B1 Group 2clarePas encore d'évaluation
- SGD LACTOSE INTOLERANCE GENETICSDocument4 pagesSGD LACTOSE INTOLERANCE GENETICSRhea Mii A CruzadoPas encore d'évaluation
- Intolerante A La LactosaDocument12 pagesIntolerante A La LactosaDaniel GarciaPas encore d'évaluation
- Lactose IntoleranceDocument26 pagesLactose IntoleranceIman ShawishPas encore d'évaluation
- Case Study Presentation: Lactose Intolerance: Central Luzon Doctors Hospital Educational InstituteDocument7 pagesCase Study Presentation: Lactose Intolerance: Central Luzon Doctors Hospital Educational InstituteGabriel FernandezPas encore d'évaluation
- What Is Lactose Intolerance and What Causes ItDocument8 pagesWhat Is Lactose Intolerance and What Causes ItElmeraine EstrellaPas encore d'évaluation
- Lactose IntoleranceDocument11 pagesLactose IntoleranceAhmed YehyaPas encore d'évaluation
- TGL 28 SPT 2012 Jam 20.00 What Is Lactose Intolerance?Document4 pagesTGL 28 SPT 2012 Jam 20.00 What Is Lactose Intolerance?y13Pas encore d'évaluation
- Lactose Intolerance or LactaseDocument2 pagesLactose Intolerance or LactaseKeth Samuel AdesasPas encore d'évaluation
- Lactose Intolerance 508 PDFDocument12 pagesLactose Intolerance 508 PDFAndi ZaidanPas encore d'évaluation
- Lactose IntoleranceDocument13 pagesLactose IntolerancelaxmiPas encore d'évaluation
- Most Human Beings Are Lactose Intolerant: Here'S Why: Arjun Walia April 3, 2013Document1 pageMost Human Beings Are Lactose Intolerant: Here'S Why: Arjun Walia April 3, 2013Prab NathanPas encore d'évaluation
- Seminar About:: Lactose IntoleranceDocument44 pagesSeminar About:: Lactose IntolerancefafaoyaPas encore d'évaluation
- Lactose Intolerance Pada AnakDocument11 pagesLactose Intolerance Pada AnakWilliam MakdinataPas encore d'évaluation
- LACTOSE INTOLERANCE by YVAN VANDENPLASDocument5 pagesLACTOSE INTOLERANCE by YVAN VANDENPLASSara Grillo MartinezPas encore d'évaluation
- O0 Lactose Intolerance 0oDocument3 pagesO0 Lactose Intolerance 0oKM TopacioPas encore d'évaluation
- Lactose Intolerance Guide: Causes, Symptoms and TestsDocument3 pagesLactose Intolerance Guide: Causes, Symptoms and TestsjoeyfongPas encore d'évaluation
- ProbióticosDocument1 pageProbióticosPatricia Alves SilvaPas encore d'évaluation
- ContentServer PDFDocument10 pagesContentServer PDFAnonymous vW8ZFJPas encore d'évaluation
- Understanding Lactose IntoleranceDocument63 pagesUnderstanding Lactose IntoleranceCarl Angelo SuaybaguioPas encore d'évaluation
- Galactosemia and Lactose Intolerance Powerpoint FinalDocument72 pagesGalactosemia and Lactose Intolerance Powerpoint FinalNico Batalla60% (5)
- Lactose IntoleranceDocument5 pagesLactose IntoleranceNader Smadi100% (1)
- Metabolism of CarbohydratesDocument26 pagesMetabolism of CarbohydratesMM Qizill50% (2)
- Lactose Intolerance GRP 7 E-1Document39 pagesLactose Intolerance GRP 7 E-1Carl Angelo Suaybaguio100% (1)
- Biochem Case.2Document22 pagesBiochem Case.2Nogra CarlPas encore d'évaluation
- Physiological Basis of Lactose Intolerance and Malabsorption SyndromeDocument8 pagesPhysiological Basis of Lactose Intolerance and Malabsorption SyndromeRownak BelkhierPas encore d'évaluation
- Lactose intolerance diagnosis and treatmentDocument12 pagesLactose intolerance diagnosis and treatmentNico BatallaPas encore d'évaluation
- MOOC on Biochemistry Module-7 Carbohydrates (Part-1Document3 pagesMOOC on Biochemistry Module-7 Carbohydrates (Part-1NihalPas encore d'évaluation
- Estudio Lactase Head StartDocument8 pagesEstudio Lactase Head StartXavier GalarzaPas encore d'évaluation
- GalactosemiaDocument9 pagesGalactosemianaziratulPas encore d'évaluation
- Abnormalities of Carbohydrate DigestionDocument12 pagesAbnormalities of Carbohydrate Digestionsuzi suziPas encore d'évaluation
- Lactose Intolerance: Tuula H. Vesa Philippe Marteau Riitta Korpela +Document31 pagesLactose Intolerance: Tuula H. Vesa Philippe Marteau Riitta Korpela +Yatinah YuPas encore d'évaluation
- ok2009LATTOSIO RIVISTALactoseintoleranceanon-allergicdisorderoftenmanagedDocument15 pagesok2009LATTOSIO RIVISTALactoseintoleranceanon-allergicdisorderoftenmanagedNixPas encore d'évaluation
- Lactose IntoleranceDocument2 pagesLactose IntoleranceJae WonPas encore d'évaluation
- Gita Aryanti 030.07.098: Faculty of Medicine Trisakti UniversityDocument39 pagesGita Aryanti 030.07.098: Faculty of Medicine Trisakti UniversitygitaaryantiPas encore d'évaluation
- PCH 201: Clinical Biochemistry Lecture Notes 2 - Lactose Intolerance and GalactosemiaDocument18 pagesPCH 201: Clinical Biochemistry Lecture Notes 2 - Lactose Intolerance and GalactosemiaKellyPas encore d'évaluation
- Difference Between Soluble Fiber and Insoluble FiberDocument5 pagesDifference Between Soluble Fiber and Insoluble FiberAngela Francesca DuranPas encore d'évaluation
- Lomer 2008 (Intolerancia A La Lactosa)Document11 pagesLomer 2008 (Intolerancia A La Lactosa)michellevcfPas encore d'évaluation
- This Is A SampleDocument10 pagesThis Is A SampleNashi TagazaPas encore d'évaluation
- Recent Diagnostic Tests for Lactose IntoleranceDocument12 pagesRecent Diagnostic Tests for Lactose IntoleranceBerlia NarayaniPas encore d'évaluation
- Enzymes-Lactose 20intoleranceDocument2 pagesEnzymes-Lactose 20intoleranceapi-323374257Pas encore d'évaluation
- Digestion and Absorption of Carbohydrates: by Arpitha 3 BnysDocument31 pagesDigestion and Absorption of Carbohydrates: by Arpitha 3 BnysBig ZeroPas encore d'évaluation
- Nutrition Bytes: TitleDocument8 pagesNutrition Bytes: TitleDayana CarrilloPas encore d'évaluation
- Lactase Lab AnswerDocument3 pagesLactase Lab AnswerSenpai ChibiPas encore d'évaluation
- LOMER Et Al-2008-Alimentary Pharmacology & Therapeutics PDFDocument11 pagesLOMER Et Al-2008-Alimentary Pharmacology & Therapeutics PDFM SPas encore d'évaluation
- Lactose Malabsorption and IntoleranceDocument20 pagesLactose Malabsorption and IntoleranceJORGE ANDRÉS BONILLA VEGAPas encore d'évaluation
- Study Case Lactose Intolerance Sofia MontoyaDocument4 pagesStudy Case Lactose Intolerance Sofia MontoyaMaría Sofía MontoyaPas encore d'évaluation
- Tessmosleyirr Docx-2Document4 pagesTessmosleyirr Docx-2api-265068297Pas encore d'évaluation
- Malabsorption SyndromeDocument6 pagesMalabsorption SyndromeIris BakerPas encore d'évaluation
- CC 1 and CC4Document26 pagesCC 1 and CC4Morgan Grace Yap PausaPas encore d'évaluation
- Lactose Intolerance: C2 - Group 3Document29 pagesLactose Intolerance: C2 - Group 3Mark PadulloPas encore d'évaluation
- Sự Tiêu Hóa Và Hấp Thụ CarbonhydrateDocument51 pagesSự Tiêu Hóa Và Hấp Thụ CarbonhydrateSỹ NguyễnPas encore d'évaluation
- The Role of Colonic Metabolism in Lactose IntoleranceDocument7 pagesThe Role of Colonic Metabolism in Lactose IntoleranceFranciele Anjos100% (1)
- Lactose Intolerance in InfantsDocument10 pagesLactose Intolerance in InfantsflorencePas encore d'évaluation
- Lactose Intolerance An Update On Its Pathogenesis, Diagnosis, and TreatmentDocument10 pagesLactose Intolerance An Update On Its Pathogenesis, Diagnosis, and TreatmentDayanaPas encore d'évaluation
- Carbohydrate Digestion NASPGHANDocument8 pagesCarbohydrate Digestion NASPGHANPradusha RevuruPas encore d'évaluation
- Lactose Intolerance A2 GRP 3Document60 pagesLactose Intolerance A2 GRP 3Kristian CadaPas encore d'évaluation
- Lactose Intolerance, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandLactose Intolerance, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Perhitungan Mutu Protein-1Document7 pagesPerhitungan Mutu Protein-1Pedina AnindyaPas encore d'évaluation
- Perhitungan Mutu ProteinDocument7 pagesPerhitungan Mutu ProteinPedina AnindyaPas encore d'évaluation
- 10 Health Benefits of AvocadosDocument2 pages10 Health Benefits of AvocadosPedina AnindyaPas encore d'évaluation
- The Skinny On SkinfoldDocument3 pagesThe Skinny On SkinfoldPedina AnindyaPas encore d'évaluation
- AntibioticsDocument2 pagesAntibioticsPedina AnindyaPas encore d'évaluation
- Interaksi Antara Obat & Herbal-EditDocument28 pagesInteraksi Antara Obat & Herbal-EditPedina AnindyaPas encore d'évaluation
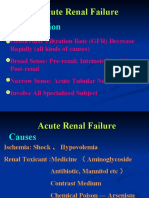
- Acte Renal FailureDocument21 pagesActe Renal Failureapi-19916399Pas encore d'évaluation
- The Nature and Meaning of Physical EducationDocument14 pagesThe Nature and Meaning of Physical EducationRegie Mark MansiguePas encore d'évaluation
- Salicylic Acid and Sulfur (Topical Route) : Commonly Used Brand Name(s)Document9 pagesSalicylic Acid and Sulfur (Topical Route) : Commonly Used Brand Name(s)Gutu DoinaPas encore d'évaluation
- Why Can'T We Just Drink The Water From Natural Sources?: Myths About Contaminated WaterDocument2 pagesWhy Can'T We Just Drink The Water From Natural Sources?: Myths About Contaminated WaterAiron Kaye SameloPas encore d'évaluation
- Benefits of An Experimental Program of Equestrian Therapy For Children With ADHD PDFDocument10 pagesBenefits of An Experimental Program of Equestrian Therapy For Children With ADHD PDFJuli DeviaPas encore d'évaluation
- Fundamentals of Caregiving Learner’s GuideDocument357 pagesFundamentals of Caregiving Learner’s GuideBfp SapangdalagaPas encore d'évaluation
- E-Learning PHARM 131 - Chapter2Document10 pagesE-Learning PHARM 131 - Chapter2Ryan Charles Uminga GalizaPas encore d'évaluation
- MIDAS QuestionnaireDocument1 pageMIDAS QuestionnaireNHFChicagoPas encore d'évaluation
- Lumbar PunctureDocument18 pagesLumbar PunctureJaspreet KangPas encore d'évaluation
- Rheumatoid Arthritis: Know Your OptionsDocument11 pagesRheumatoid Arthritis: Know Your OptionsMartin UllielPas encore d'évaluation
- DLL Health Grade8 Quarter4 Palawan DivisionDocument9 pagesDLL Health Grade8 Quarter4 Palawan Divisionemitz Jun ventura100% (5)
- Optimizing Active Case-Finding For Tuberculosis: Implementation Lessons From South-East AsiaDocument97 pagesOptimizing Active Case-Finding For Tuberculosis: Implementation Lessons From South-East AsiaRisdi PramestaPas encore d'évaluation
- Professional Adjustment, Leadership-Management Post-Test Set ADocument7 pagesProfessional Adjustment, Leadership-Management Post-Test Set AYaj CruzadaPas encore d'évaluation
- Medifocus April 2007Document61 pagesMedifocus April 2007Pushpanjali Crosslay HospitalPas encore d'évaluation
- Action Plan On Medical and Nursing: Resource ReqmtsDocument15 pagesAction Plan On Medical and Nursing: Resource ReqmtsJude Mathew100% (2)
- Neonatal Glycaemia and Neurodevelopmental Outcomes A Systematic Review and Meta Analysis.Document11 pagesNeonatal Glycaemia and Neurodevelopmental Outcomes A Systematic Review and Meta Analysis.Alma Iris Rodriguez D PadillaPas encore d'évaluation
- 2016 - Are There Subconcussive Neuropsychological Effects in Youth Sports? An Exploratory Study of High - and Low-Contact SportsDocument8 pages2016 - Are There Subconcussive Neuropsychological Effects in Youth Sports? An Exploratory Study of High - and Low-Contact SportsRaúl VerdugoPas encore d'évaluation
- 2021 Global Provider Manual - v4-3Document1 page2021 Global Provider Manual - v4-3Corporate PA Progress GroupPas encore d'évaluation
- FCA FormatDocument4 pagesFCA FormatAlexa PasionPas encore d'évaluation
- Neonates: Clinical Syndromes and Cardinal Fea-Tures of Infectious Diseases: Approach To Diagnosis and Initial ManagementDocument7 pagesNeonates: Clinical Syndromes and Cardinal Fea-Tures of Infectious Diseases: Approach To Diagnosis and Initial ManagementFatma ElzaytPas encore d'évaluation
- MSW Syllabus Semester WiseDocument3 pagesMSW Syllabus Semester WisepalprakahPas encore d'évaluation
- 9 Wireframe DocumentDocument7 pages9 Wireframe Documentharshaddanawale.nbnssoe.compPas encore d'évaluation
- Danone Integrated Annual Report 2021Document40 pagesDanone Integrated Annual Report 2021mohit gedamPas encore d'évaluation
- The ADHD Diagnosis GuideDocument13 pagesThe ADHD Diagnosis GuideArunima KapoorPas encore d'évaluation
- The Plant Paradox: The Hidden Dangers in "Healthy" Foods That Cause Disease and Weight Gain - Dr. Steven R Gundry MDDocument5 pagesThe Plant Paradox: The Hidden Dangers in "Healthy" Foods That Cause Disease and Weight Gain - Dr. Steven R Gundry MDrugywine15% (13)
- ACF Community Nutrition GuideDocument170 pagesACF Community Nutrition GuideAction Against Hunger USA100% (1)
- Scoring The Survey: Maysi 2 Scoringkey ScoringkeyDocument11 pagesScoring The Survey: Maysi 2 Scoringkey Scoringkey7 MNTPas encore d'évaluation
- Answer Key CicDocument3 pagesAnswer Key Cictiburshoc16Pas encore d'évaluation
- Iliotibial Band Syndrome - FannyDocument13 pagesIliotibial Band Syndrome - FannyAlfiani Rosyida Arisanti Syafi'iPas encore d'évaluation
- Nitric Acid 70%Document10 pagesNitric Acid 70%Oscar ValdezPas encore d'évaluation