Vous aimerez peut-être aussi
- Building A Tesla Turbine From Hard Drive PlattersDocument7 pagesBuilding A Tesla Turbine From Hard Drive PlattersebonPas encore d'évaluation
- Chinese Character Writing Exercise SheetsDocument47 pagesChinese Character Writing Exercise Sheetsapi-3700050100% (1)
- Climbing Robots in Natural Terrain: KeywordsDocument8 pagesClimbing Robots in Natural Terrain: KeywordsNagesh BheemaPas encore d'évaluation
- BRUNI 2012 Wells-120517-DsDocument22 pagesBRUNI 2012 Wells-120517-DsebonPas encore d'évaluation
- TP 112Document8 pagesTP 112ebonPas encore d'évaluation
- El Año NuevoDocument1 pageEl Año NuevoebonPas encore d'évaluation
- Day For RememberDocument1 pageDay For RememberebonPas encore d'évaluation
- Pink MoonDocument1 pagePink MoonebonPas encore d'évaluation
- Mem ForgetDocument1 pageMem ForgetebonPas encore d'évaluation
- Pink SunDocument1 pagePink SunebonPas encore d'évaluation
- GWWCDocument48 pagesGWWCebonPas encore d'évaluation
- Hand Powered Water PumpsDocument25 pagesHand Powered Water PumpsFredrik GaddPas encore d'évaluation
- At Elec P Ei Steps Xe Archimedesworksheet2012Document4 pagesAt Elec P Ei Steps Xe Archimedesworksheet2012ebonPas encore d'évaluation
- A Complete Illustrated Guide To The PC HardwareDocument240 pagesA Complete Illustrated Guide To The PC HardwareKarthikFriendPas encore d'évaluation
- Guide To Private WellsDocument33 pagesGuide To Private WellsebonPas encore d'évaluation
- Skoda Fabia 2000 MaintenanceDocument86 pagesSkoda Fabia 2000 Maintenancebambimbam75% (4)
- The Blue Bells of Scotland: C G/D DM em F C/G C G7 C/E CDocument2 pagesThe Blue Bells of Scotland: C G/D DM em F C/G C G7 C/E CebonPas encore d'évaluation
- Design of A Low-Cost Drilling RigDocument92 pagesDesign of A Low-Cost Drilling RigstarspleshPas encore d'évaluation
- The Fingering Problem 5 PreCDocument35 pagesThe Fingering Problem 5 PreCapi-3731582Pas encore d'évaluation
- BRUNI 2012 Wells-120517-DsDocument22 pagesBRUNI 2012 Wells-120517-DsebonPas encore d'évaluation
- AA Drilling ManualDocument45 pagesAA Drilling ManualebonPas encore d'évaluation
- Ctis-Ttom SyllabusDocument5 pagesCtis-Ttom SyllabusebonPas encore d'évaluation
- Bit Coin PresentationDocument77 pagesBit Coin PresentationebonPas encore d'évaluation
- SFAStirling Engine TemplatesDocument4 pagesSFAStirling Engine TemplatesEl GronePas encore d'évaluation
- Bitcoin BookDocument70 pagesBitcoin BookebonPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Tripetala) and Its Use As Substitute For Ginger in ZoboDocument9 pagesTripetala) and Its Use As Substitute For Ginger in Zobocicilya_yulianaPas encore d'évaluation
- Defects in Butter..gyarsilal Yadav PDFDocument28 pagesDefects in Butter..gyarsilal Yadav PDFprahalad yadav100% (1)
- CUL 1101 Culinary Terms and Cooking MethodsDocument1 pageCUL 1101 Culinary Terms and Cooking MethodsBryan FongPas encore d'évaluation
- Home Economics Appetizers & DessertsDocument2 pagesHome Economics Appetizers & DessertsKISHAPas encore d'évaluation
- 8aa NutritionDocument29 pages8aa NutritionmaryamPas encore d'évaluation
- St. Paul's College Lunch Menu Nov 2022Document2 pagesSt. Paul's College Lunch Menu Nov 2022djakwdkjnPas encore d'évaluation
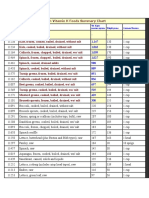
- High Vitamin K Foods Summary ChartDocument35 pagesHigh Vitamin K Foods Summary ChartNurul Huda 귀여운Pas encore d'évaluation
- SMP KLT - BAHASA INGGRIS SoalDocument7 pagesSMP KLT - BAHASA INGGRIS SoalYuarina HadiPas encore d'évaluation
- The Awareness of Fast Food Among StudentDocument8 pagesThe Awareness of Fast Food Among StudentCarlsonCarlPas encore d'évaluation
- 2010-Jan-14 Malunggay Recipe Book PDFDocument108 pages2010-Jan-14 Malunggay Recipe Book PDFdayle0282% (11)
- IELTS 03 - Listening 03 & Reading 03 - Transcripts & KeysDocument7 pagesIELTS 03 - Listening 03 & Reading 03 - Transcripts & KeysLe Hoang KhaPas encore d'évaluation
- Ingles 1er Bchto U 4 - M4Document8 pagesIngles 1er Bchto U 4 - M4Esmeralda Ruano100% (1)
- Hs 10.2.1 Section 2 HaccpDocument20 pagesHs 10.2.1 Section 2 HaccpKhaled SaidPas encore d'évaluation
- Cooking Meals According to RecipesDocument15 pagesCooking Meals According to RecipesChristelle Joy Cordero100% (3)
- Picazzos Take Out Menu 2018 12 15 2018Document2 pagesPicazzos Take Out Menu 2018 12 15 2018LeahPas encore d'évaluation
- Global HungerDocument35 pagesGlobal HungerJANMATTHEW PAPAPas encore d'évaluation
- Business Plan Final 1Document17 pagesBusiness Plan Final 1Sarah Asher LegaspiPas encore d'évaluation
- DinnerDocument2 pagesDinnereatlocalmenusPas encore d'évaluation
- Charcuterie 9781439069936Document368 pagesCharcuterie 9781439069936Thalyta Cruxz100% (6)
- Cantonese Soy Sauce Fried Noodles RecipeDocument3 pagesCantonese Soy Sauce Fried Noodles RecipeClark RebusquilloPas encore d'évaluation
- Formation of Societies: From Hunting and Gathering to Food ProductionDocument32 pagesFormation of Societies: From Hunting and Gathering to Food ProductionmnbvhPas encore d'évaluation
- 1-Introduction To CookeryDocument26 pages1-Introduction To CookeryEdchel Espeña100% (2)
- Family daily routinesDocument2 pagesFamily daily routinesDAZA MONTAÑA ANDRES CAMILOPas encore d'évaluation
- Cookery 10: Technology and Livelihood Education Learning Activity Sheet (Q4 - Week 1)Document4 pagesCookery 10: Technology and Livelihood Education Learning Activity Sheet (Q4 - Week 1)Angeline Cortez100% (1)
- Shri Umesh HebbarDocument74 pagesShri Umesh Hebbars.sabapathyPas encore d'évaluation
- Pes Statement WorksheetDocument2 pagesPes Statement Worksheetapi-638539712Pas encore d'évaluation
- Kamias JamDocument5 pagesKamias JamFerjeanie Bernandino50% (2)
- Revised Hamper PDFDocument28 pagesRevised Hamper PDFADITAPas encore d'évaluation
- Business Plan Group 4 10 CDocument3 pagesBusiness Plan Group 4 10 CBYUanime PHPas encore d'évaluation
- Potensi Limbah Padi Sebagai Pakan Sapi B c4151c3fDocument7 pagesPotensi Limbah Padi Sebagai Pakan Sapi B c4151c3fPartai Kunam SejahteraPas encore d'évaluation