Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Risk Assessment of Heavy LiftingDocument5 pagesRisk Assessment of Heavy Lifting채종언100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Evidence-Based Practice in Pediatric Physical Therapy by BarryDocument14 pagesEvidence-Based Practice in Pediatric Physical Therapy by BarryFe TusPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- FWA CMS Training (4346) PDFDocument13 pagesFWA CMS Training (4346) PDFinfo3497Pas encore d'évaluation
- Personality Disorders PDFDocument35 pagesPersonality Disorders PDFABHINAVPas encore d'évaluation
- ACOG - External Cephalic Version PDFDocument10 pagesACOG - External Cephalic Version PDFPat CabanitPas encore d'évaluation
- The Impact of Longitudinal Studies On Understanding Development From Young Adulthood To Old AgeDocument11 pagesThe Impact of Longitudinal Studies On Understanding Development From Young Adulthood To Old AgeLana PeharPas encore d'évaluation
- HLTWHS002 AE KN 1of3 Katarina JosipovicDocument20 pagesHLTWHS002 AE KN 1of3 Katarina Josipovicwriter top100% (1)
- Week 2 SolutionsDocument4 pagesWeek 2 Solutionsannavarapuanand100% (2)
- Different Committees in The HospitalDocument8 pagesDifferent Committees in The HospitalShehnaz SheikhPas encore d'évaluation
- Letters of Intent (Cover Letters)Document6 pagesLetters of Intent (Cover Letters)anca_ramona_s0% (1)
- NCP Impaired Gas Exhange Related To Alveolar Wall Destruction EMPHYSEMADocument5 pagesNCP Impaired Gas Exhange Related To Alveolar Wall Destruction EMPHYSEMAMa. Elaine Carla Tating50% (2)
- 7 Legal Dimensions of Nursing Chapter ReviewDocument2 pages7 Legal Dimensions of Nursing Chapter ReviewAmy AnonymousPas encore d'évaluation
- FA CPR Workbook 0001Document56 pagesFA CPR Workbook 0001Shawn KimballPas encore d'évaluation
- Providing Information Raising Awareness: June 2015Document17 pagesProviding Information Raising Awareness: June 2015Aymanahmad AymanPas encore d'évaluation
- Tipos de Diabetes - Diabetes MonogenicaDocument27 pagesTipos de Diabetes - Diabetes MonogenicaSara AmorimPas encore d'évaluation
- Domestic Violence Cycle of Violence Types of Families-2Document22 pagesDomestic Violence Cycle of Violence Types of Families-2api-340420872Pas encore d'évaluation
- Safety Pocket Guide Web 061808Document534 pagesSafety Pocket Guide Web 061808hombre911100% (1)
- Ecological Analysis of The Prevalence of PulmonaryDocument10 pagesEcological Analysis of The Prevalence of PulmonaryLazy SlothPas encore d'évaluation
- 20 MG 100 ML ConivaptanDocument18 pages20 MG 100 ML Conivaptanahmedradwan2005Pas encore d'évaluation
- MDMA-assisted Therapy Significantly Reduces Eating Disorder Symptoms in A Randomized Placebo-Controlled Trial of Adults With Severe PTSDDocument8 pagesMDMA-assisted Therapy Significantly Reduces Eating Disorder Symptoms in A Randomized Placebo-Controlled Trial of Adults With Severe PTSDKayla GreenstienPas encore d'évaluation
- Alternatives To Hydrazine MHI PaperDocument5 pagesAlternatives To Hydrazine MHI PaperjycortesPas encore d'évaluation
- Position Paper de l'UEFA Sur L'interdiction Du Gazon Synthétique Par l'ECHA 19 Juillet 2019Document8 pagesPosition Paper de l'UEFA Sur L'interdiction Du Gazon Synthétique Par l'ECHA 19 Juillet 2019LeMonde.frPas encore d'évaluation
- Asthma Case StudyDocument39 pagesAsthma Case StudyDimitris TasiouPas encore d'évaluation
- Lab Report 15438869 20231127064225Document1 pageLab Report 15438869 20231127064225carilloabhe21Pas encore d'évaluation
- CephalosporinsDocument20 pagesCephalosporinsBianca Andrea RagazaPas encore d'évaluation
- DENGUEDocument17 pagesDENGUEPramod LamichhanePas encore d'évaluation
- Prescribing For Transgender Patients ELHEDocument4 pagesPrescribing For Transgender Patients ELHEGe YgayPas encore d'évaluation
- Lista Medicamente OTC Conform Nomenclator ANM 17 Feb2020Document184 pagesLista Medicamente OTC Conform Nomenclator ANM 17 Feb2020Andreea PasolPas encore d'évaluation
- Prilosec (Omeprazole) MoreDocument3 pagesPrilosec (Omeprazole) MoreLuis Arturo Andrade CoronadoPas encore d'évaluation
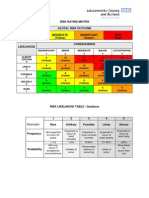
- Example of A NHS Risk Rating MatrixDocument2 pagesExample of A NHS Risk Rating MatrixRochady SetiantoPas encore d'évaluation