Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Operational Business Suite Contract by SSNIT Signed in 2012Document16 pagesOperational Business Suite Contract by SSNIT Signed in 2012GhanaWeb EditorialPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Splunk Certification: Certification Exam Study GuideDocument18 pagesSplunk Certification: Certification Exam Study GuidesalemselvaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Thermo King Tool Catalog Part 2Document53 pagesThermo King Tool Catalog Part 2Alb NewgatePas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- SAN MIGUEL CORPORATION, ANGEL G. ROA and MELINDA MACARAIG, vs. NATIONAL LABOR RELATIONS COMMISSION (Second Division), LABOR ARBITER EDUARDO J. CARPIO, ILAW AT BUKLOD NG MANGGAGAWA (IBM), ET ALDocument6 pagesSAN MIGUEL CORPORATION, ANGEL G. ROA and MELINDA MACARAIG, vs. NATIONAL LABOR RELATIONS COMMISSION (Second Division), LABOR ARBITER EDUARDO J. CARPIO, ILAW AT BUKLOD NG MANGGAGAWA (IBM), ET ALLaila Ismael SalisaPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Data Loss PreventionDocument20 pagesData Loss Preventiondeepak4315Pas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Modeling Cover Letter No ExperienceDocument7 pagesModeling Cover Letter No Experienceimpalayhf100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Geotechnical Design MannulDocument828 pagesGeotechnical Design MannulJie ZhouPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
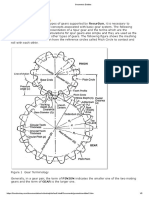
- Geometric Entities: Basic Gear TerminologyDocument5 pagesGeometric Entities: Basic Gear TerminologyMatija RepincPas encore d'évaluation
- On Fracture MechanicsDocument81 pagesOn Fracture MechanicsDEEPAK100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Beijing-Michael PageDocument71 pagesBeijing-Michael Pagejohndavsg8022Pas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Managerial Economics - 1Document36 pagesManagerial Economics - 1Deepi SinghPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hydraulic Breakers in Mining ApplicationDocument28 pagesHydraulic Breakers in Mining ApplicationdrmassterPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Oxford Handbooks Online: From Old To New Developmentalism in Latin AmericaDocument27 pagesOxford Handbooks Online: From Old To New Developmentalism in Latin AmericadiegoPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Vitus Bering, Centre For Higher Education: Jens Bertelsen & Jens Peder PedersenDocument50 pagesVitus Bering, Centre For Higher Education: Jens Bertelsen & Jens Peder PedersenAnca IscruPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- 1.2 Installation of SSH Keys On Linux-A Step-By Step GuideDocument3 pages1.2 Installation of SSH Keys On Linux-A Step-By Step GuideMada ChouchouPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Ara FormDocument2 pagesAra Formjerish estemPas encore d'évaluation
- BSNL Project MBA NitishDocument92 pagesBSNL Project MBA NitishAnkitSingh0% (2)
- Reaching Different Learning Styles ThrouDocument29 pagesReaching Different Learning Styles ThrouKENNETH HERRERAPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- 1 Introduction To Pharmaceutical Dosage Forms Part1Document32 pages1 Introduction To Pharmaceutical Dosage Forms Part1Joanna Carla Marmonejo Estorninos-Walker100% (1)
- Burndown Sample ClayDocument64 pagesBurndown Sample ClaybluemaxPas encore d'évaluation
- Definition of Sustainable Packaging PDFDocument10 pagesDefinition of Sustainable Packaging PDFProf C.S.PurushothamanPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
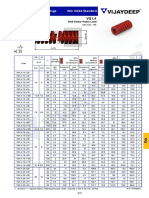
- Rectangular Wire Die Springs ISO-10243 Standard: Red Colour Heavy LoadDocument3 pagesRectangular Wire Die Springs ISO-10243 Standard: Red Colour Heavy LoadbashaPas encore d'évaluation
- Unilever Financial PerformanceDocument9 pagesUnilever Financial PerformanceAbdul QayumPas encore d'évaluation
- KEC International Limited: Pile FoundationDocument49 pagesKEC International Limited: Pile FoundationDinesh Kumar100% (1)
- Octopus 900 Instructions For UseDocument18 pagesOctopus 900 Instructions For UseAli FadhilPas encore d'évaluation
- 11 - Savulescu Et Al (2020) - Equality or Utility. Ethics and Law of Rationing VentilatorsDocument6 pages11 - Savulescu Et Al (2020) - Equality or Utility. Ethics and Law of Rationing VentilatorsCorrado BisottoPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- KINDRED HEALTHCARE, INC 10-K (Annual Reports) 2009-02-25Document329 pagesKINDRED HEALTHCARE, INC 10-K (Annual Reports) 2009-02-25http://secwatch.comPas encore d'évaluation
- Philips Chassis Lc4.31e Aa Power Dps 181 PDFDocument9 pagesPhilips Chassis Lc4.31e Aa Power Dps 181 PDFAouadi AbdellazizPas encore d'évaluation
- ABAP On HANA Interview QuestionsDocument26 pagesABAP On HANA Interview QuestionsNagesh reddyPas encore d'évaluation
- BON Resolution No 08 1994Document2 pagesBON Resolution No 08 1994Noel100% (9)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)