Vous aimerez peut-être aussi
- The Anti-PaladinDocument9 pagesThe Anti-PaladinBobbyPas encore d'évaluation
- Domesticity and Power in The Early Mughal WorldDocument17 pagesDomesticity and Power in The Early Mughal WorldUjjwal Gupta100% (1)
- Fracture in Leg Tibia and FibulaDocument27 pagesFracture in Leg Tibia and Fibulachilsya shajiPas encore d'évaluation
- Varus Knee Classification and CorrectionDocument8 pagesVarus Knee Classification and CorrectionPraharshaPas encore d'évaluation
- Ligamentous Injuries About The Ankle and Subtalar Joints: Hans Zwipp, MD, PHD, Stefan Rammelt, MD, Rene Grass, MDDocument35 pagesLigamentous Injuries About The Ankle and Subtalar Joints: Hans Zwipp, MD, PHD, Stefan Rammelt, MD, Rene Grass, MDAnonymous kdBDppigEPas encore d'évaluation
- Affidavit of Co OwnershipDocument2 pagesAffidavit of Co OwnershipEmer MartinPas encore d'évaluation
- Ankle Syndesmotic InjuryDocument10 pagesAnkle Syndesmotic InjuryC Martin TraumatoPas encore d'évaluation
- Full Denture ProstheticDocument6 pagesFull Denture ProstheticAndykaYayanSetiawanPas encore d'évaluation
- Ankle Fractures: A Literature Review of Current Treatment MethodsDocument13 pagesAnkle Fractures: A Literature Review of Current Treatment Methodsadrian1989Pas encore d'évaluation
- Actures of The Midfoot and ForefootDocument37 pagesActures of The Midfoot and ForefootMrHadezz LamerPas encore d'évaluation
- OB and Attendance PolicyDocument2 pagesOB and Attendance PolicyAshna MeiPas encore d'évaluation
- Oral N Maxilofacial Surgery PDFDocument9 pagesOral N Maxilofacial Surgery PDFAndykaYayanSetiawanPas encore d'évaluation
- Oral N Maxilofacial Surgery PDFDocument9 pagesOral N Maxilofacial Surgery PDFAndykaYayanSetiawanPas encore d'évaluation
- Ankle Syndesmosis InjuriesDocument16 pagesAnkle Syndesmosis InjuriesRin MaghfirahPas encore d'évaluation
- Bonded Composites Versus Ceramic Veneers PDFDocument7 pagesBonded Composites Versus Ceramic Veneers PDFAndykaYayanSetiawanPas encore d'évaluation
- Inside Outside Bleaching Technique - Poyser NJ, Kelleher MGD PDFDocument8 pagesInside Outside Bleaching Technique - Poyser NJ, Kelleher MGD PDFAndykaYayanSetiawanPas encore d'évaluation
- S-Sapfico-Satyanarayanamaterial 121212Document183 pagesS-Sapfico-Satyanarayanamaterial 121212mpsing1133Pas encore d'évaluation
- B-GL-385-009 Short Range Anti-Armour Weapon (Medium)Document171 pagesB-GL-385-009 Short Range Anti-Armour Weapon (Medium)Jared A. Lang100% (1)
- Musculoskeletal Radiology NotesDocument62 pagesMusculoskeletal Radiology Notesmeshmatic1234567100% (3)
- Investigation Data FormDocument1 pageInvestigation Data Formnildin danaPas encore d'évaluation
- Eular Us Course Modulo 5 Tornozelo e PeDocument44 pagesEular Us Course Modulo 5 Tornozelo e PeGustavo Bernardo DamascenoPas encore d'évaluation
- 10 1007@s00068-mfjrbtDocument14 pages10 1007@s00068-mfjrbtJGunar VasquezPas encore d'évaluation
- Proximal Tibial Fractures in AdultsDocument4 pagesProximal Tibial Fractures in AdultsAbdusSomadPas encore d'évaluation
- Tugas ReconstructionDocument13 pagesTugas ReconstructionReza Devianto HambaliPas encore d'évaluation
- Clinical Anatomy of The Knee PDFDocument7 pagesClinical Anatomy of The Knee PDFJuan Victor Briceno OrtizPas encore d'évaluation
- Rehabilitation of Knee Injuries: Robert C. Manske and Mark V. PaternoDocument23 pagesRehabilitation of Knee Injuries: Robert C. Manske and Mark V. PaternoYMatosPas encore d'évaluation
- Pic RenderDocument7 pagesPic RenderMo GomaaPas encore d'évaluation
- Torsion of The Human Achilles Tendon JFAS 1996Document11 pagesTorsion of The Human Achilles Tendon JFAS 1996Evan BowlesPas encore d'évaluation
- Ankle Fractures in Adults - UpToDateDocument50 pagesAnkle Fractures in Adults - UpToDateJose LuceroPas encore d'évaluation
- Fracturas de La Porción Media Del Húmero en Adultos - UpToDateDocument37 pagesFracturas de La Porción Media Del Húmero en Adultos - UpToDateRogelio MoscosoPas encore d'évaluation
- Pathologic Afflictions of The Achilles Tendon JFAS 1991Document8 pagesPathologic Afflictions of The Achilles Tendon JFAS 1991Evan BowlesPas encore d'évaluation
- Shaft Femur FracturesDocument75 pagesShaft Femur FracturesRudi MihaiPas encore d'évaluation
- Azar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureDocument4 pagesAzar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureKuozram No MasPas encore d'évaluation
- 1 s2.0 S1877056819302713 MainDocument12 pages1 s2.0 S1877056819302713 MainMarianoPas encore d'évaluation
- Tennis Leg Gastrocnemius Injury Is A Far More Comm-1Document4 pagesTennis Leg Gastrocnemius Injury Is A Far More Comm-1jasonoytumandukPas encore d'évaluation
- A) The Anatomy in Relation To Injury of The Lateral Collateral Ligaments of The Ankle PDFDocument8 pagesA) The Anatomy in Relation To Injury of The Lateral Collateral Ligaments of The Ankle PDFericdgPas encore d'évaluation
- Gadline PrsentationDocument12 pagesGadline PrsentationsumardiPas encore d'évaluation
- Taro 2016 ComentadoDocument42 pagesTaro 2016 ComentadoneossmedPas encore d'évaluation
- RCT PROJECT WORK FullDocument94 pagesRCT PROJECT WORK FulliquramasiddiquePas encore d'évaluation
- Fracturas de TobilloDocument23 pagesFracturas de TobilloGregorio VillarrealPas encore d'évaluation
- Anatomy and PhysiologyDocument4 pagesAnatomy and PhysiologySarah CabalquintoPas encore d'évaluation
- Anatomi AnkleDocument15 pagesAnatomi AnkleZera DirgantaraPas encore d'évaluation
- Mri Evaluation of Shoulder Joint: Normal Anatomy & Pathological Finding A Pictorial Essay and ReviewDocument9 pagesMri Evaluation of Shoulder Joint: Normal Anatomy & Pathological Finding A Pictorial Essay and ReviewIqhe Harsono SyastrowinotoPas encore d'évaluation
- High Ankle Sprain in Athletes Diagnostic Challenges and Review of The LiteratureDocument9 pagesHigh Ankle Sprain in Athletes Diagnostic Challenges and Review of The LiteratureOscar NgPas encore d'évaluation
- Chronic Tibiofibular DiastasisDocument13 pagesChronic Tibiofibular DiastasisDebangshu KumarPas encore d'évaluation
- 10.1177 1941738110397875 PDFDocument16 pages10.1177 1941738110397875 PDFalwy sugiartoPas encore d'évaluation
- Anatomical Arthroscopic Graft Reconstruction of The Anterior Tibiofibular Ligament For Chronic Disruption of The Distal SyndesmosisDocument5 pagesAnatomical Arthroscopic Graft Reconstruction of The Anterior Tibiofibular Ligament For Chronic Disruption of The Distal SyndesmosisMoustafa MohamedPas encore d'évaluation
- MDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewDocument9 pagesMDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewcalinmariusPas encore d'évaluation
- Anatomia Clinica KneeDocument17 pagesAnatomia Clinica KneeMauricio OjedaPas encore d'évaluation
- Bab 1Document12 pagesBab 1ibnu syahPas encore d'évaluation
- Musculoskeletal MSK X-Ray Interpretation OSCE GuideDocument9 pagesMusculoskeletal MSK X-Ray Interpretation OSCE GuideKru PrimePas encore d'évaluation
- 8 Ankle SprainDocument11 pages8 Ankle Sprainapi-241264935Pas encore d'évaluation
- Postero Lateral Corner of KneeDocument5 pagesPostero Lateral Corner of KneeAnwar MarthyaPas encore d'évaluation
- Peri Articular Diseases of The Hip EmergDocument11 pagesPeri Articular Diseases of The Hip EmergwladjaPas encore d'évaluation
- 19 Tibial NerveDocument38 pages19 Tibial Nerverodrigocorcino899959Pas encore d'évaluation
- Arthroscopic Debridement and Drilling of Osteochondral Lesions of The TalusDocument15 pagesArthroscopic Debridement and Drilling of Osteochondral Lesions of The TalusAnonymous kdBDppigEPas encore d'évaluation
- Literature ReviewsDocument16 pagesLiterature ReviewssyahmibestPas encore d'évaluation
- Calcaneal Avulsion Fractures: An Often Forgotten Diagnosis: Sarah M. Yu Joseph S. YuDocument7 pagesCalcaneal Avulsion Fractures: An Often Forgotten Diagnosis: Sarah M. Yu Joseph S. YuYuni AngrianiPas encore d'évaluation
- Neer Classification - How Do We Use It and Why Is It Important?Document46 pagesNeer Classification - How Do We Use It and Why Is It Important?endy ahmaruzamryPas encore d'évaluation
- The Lisfranc JointDocument14 pagesThe Lisfranc Jointharo.r9524Pas encore d'évaluation
- Intertrochanteric Hip Fractures PDFDocument9 pagesIntertrochanteric Hip Fractures PDFSivaneasan KandiahPas encore d'évaluation
- 2016 Article 9341 PDFDocument8 pages2016 Article 9341 PDFJulenda CintarinovaPas encore d'évaluation
- Heel Spur Formation and The Subcalcaneal Enthesis of The Plantar FasciaDocument3 pagesHeel Spur Formation and The Subcalcaneal Enthesis of The Plantar FasciaanurPas encore d'évaluation
- Extensor Apparatus - AOFAS (Dalmau-Pastor)Document13 pagesExtensor Apparatus - AOFAS (Dalmau-Pastor)lukejones_85Pas encore d'évaluation
- (MRI) Bone Abnormalities of The KneeDocument11 pages(MRI) Bone Abnormalities of The KneeyPas encore d'évaluation
- Ultrasound Guided Interventional Procedures In.5Document10 pagesUltrasound Guided Interventional Procedures In.5m.lagruaPas encore d'évaluation
- ArtosDocument22 pagesArtosRia Rahmadiyani IIPas encore d'évaluation
- MonteggiaDocument14 pagesMonteggiaLPt Eka Pramiari0% (1)
- The Anatomy of The Anterior Cruciate Ligament and Its Relevance To The Technique of ReconstructionDocument7 pagesThe Anatomy of The Anterior Cruciate Ligament and Its Relevance To The Technique of ReconstructionMetin HakkanPas encore d'évaluation
- Clinical Data Fisiotek HP2Document28 pagesClinical Data Fisiotek HP2Alexandra NadinnePas encore d'évaluation
- Veener Case ReportDocument8 pagesVeener Case ReportyerrioPas encore d'évaluation
- Analisis Insiden Menggunakan RCADocument34 pagesAnalisis Insiden Menggunakan RCAAndykaYayanSetiawanPas encore d'évaluation
- 6 C 5 BDocument5 pages6 C 5 BAndykaYayanSetiawanPas encore d'évaluation
- Clinical Sheet Oral and Maxillofacial Surgery: Azienda Ospedaliera Universitaria IntegrataDocument2 pagesClinical Sheet Oral and Maxillofacial Surgery: Azienda Ospedaliera Universitaria IntegrataAndykaYayanSetiawanPas encore d'évaluation
- Regenerativ Medicine in Oral and Maxilo PDFDocument6 pagesRegenerativ Medicine in Oral and Maxilo PDFAndykaYayanSetiawanPas encore d'évaluation
- Jcedv 6 I 1 P 66Document8 pagesJcedv 6 I 1 P 66Christine HachePas encore d'évaluation
- Surgical Periodontal Theraphy Without Initial Scalling and Root PlaningDocument8 pagesSurgical Periodontal Theraphy Without Initial Scalling and Root PlaningAndykaYayanSetiawanPas encore d'évaluation
- Midline Diastema Closure With Partial Laminate Veneers: A Case ReportDocument4 pagesMidline Diastema Closure With Partial Laminate Veneers: A Case ReportAndykaYayanSetiawanPas encore d'évaluation
- Putty TeknikDocument1 pagePutty TeknikAndykaYayanSetiawanPas encore d'évaluation
- Clinical Sheet Oral and Maxillofacial Surgery: Azienda Ospedaliera Universitaria IntegrataDocument2 pagesClinical Sheet Oral and Maxillofacial Surgery: Azienda Ospedaliera Universitaria IntegrataAndykaYayanSetiawanPas encore d'évaluation
- Veneer Classification .PDGDocument10 pagesVeneer Classification .PDGAndykaYayanSetiawanPas encore d'évaluation
- Veneer Classification .PDGDocument10 pagesVeneer Classification .PDGAndykaYayanSetiawanPas encore d'évaluation
- Vital Tooth Bleaching An Update by StrasslerDocument12 pagesVital Tooth Bleaching An Update by StrassleranjozzPas encore d'évaluation
- 1 F 28Document8 pages1 F 28AndykaYayanSetiawanPas encore d'évaluation
- The Interaction of Osteoblasts With Bone-Implant Materials: 1. The Effect of Physicochemical Surface Properties of Implant MaterialsDocument17 pagesThe Interaction of Osteoblasts With Bone-Implant Materials: 1. The Effect of Physicochemical Surface Properties of Implant MaterialsAndykaYayanSetiawanPas encore d'évaluation
- B9036Document10 pagesB9036AndykaYayanSetiawanPas encore d'évaluation
- Effect of BioaggregateDocument4 pagesEffect of BioaggregateAndykaYayanSetiawanPas encore d'évaluation
- Clareamento - Resposta InflamatoriaDocument9 pagesClareamento - Resposta InflamatoriaIsabela BergerPas encore d'évaluation
- B. Partial Denture ClinicalDocument15 pagesB. Partial Denture ClinicalAndykaYayanSetiawanPas encore d'évaluation
- Fearon PDFDocument9 pagesFearon PDFAndykaYayanSetiawanPas encore d'évaluation
- DentalDocument5 pagesDentalAndykaYayanSetiawanPas encore d'évaluation
- Tooth Whitening: Efficacy, Effects and Biological SafetyDocument6 pagesTooth Whitening: Efficacy, Effects and Biological SafetyAndykaYayanSetiawanPas encore d'évaluation
- Gange - The Proper Steps To Bonding Success PDFDocument18 pagesGange - The Proper Steps To Bonding Success PDFBennyPas encore d'évaluation
- 10 1 1 897 7962Document62 pages10 1 1 897 7962AndykaYayanSetiawanPas encore d'évaluation
- Pharmacotherapy of StrokeDocument37 pagesPharmacotherapy of StrokeAndykaYayanSetiawanPas encore d'évaluation
- The Intel 8086 / 8088/ 80186 / 80286 / 80386 / 80486 Jump InstructionsDocument3 pagesThe Intel 8086 / 8088/ 80186 / 80286 / 80386 / 80486 Jump InstructionsalexiouconPas encore d'évaluation
- Acceptable Use Policy 08 19 13 Tia HadleyDocument2 pagesAcceptable Use Policy 08 19 13 Tia Hadleyapi-238178689Pas encore d'évaluation
- Flipkart Labels 06 Jul 2022 09 52Document37 pagesFlipkart Labels 06 Jul 2022 09 52Dharmesh ManiyaPas encore d'évaluation
- 02 CT311 Site WorksDocument26 pages02 CT311 Site Worksshaweeeng 101Pas encore d'évaluation
- BSRM Ultima BrochureDocument2 pagesBSRM Ultima BrochuresaifuzzamanPas encore d'évaluation
- CandyDocument24 pagesCandySjdb FjfbPas encore d'évaluation
- JEE Mains Paper 1 (12 Apr 2019 Shift 2) EnglishDocument131 pagesJEE Mains Paper 1 (12 Apr 2019 Shift 2) EnglishRudraksha KushwahaPas encore d'évaluation
- LU 5.1 ElectrochemistryDocument32 pagesLU 5.1 ElectrochemistryNurAkila Mohd YasirPas encore d'évaluation
- Vendor Registration FormDocument4 pagesVendor Registration FormhiringPas encore d'évaluation
- Ode To The West WindDocument4 pagesOde To The West WindCharis Mae DimaculanganPas encore d'évaluation
- Ferobide Applications Brochure English v1 22Document8 pagesFerobide Applications Brochure English v1 22Thiago FurtadoPas encore d'évaluation
- MegaMacho Drums BT READ MEDocument14 pagesMegaMacho Drums BT READ MEMirkoSashaGoggoPas encore d'évaluation
- 1572 - Anantha Narayanan FFS CalculationDocument1 page1572 - Anantha Narayanan FFS CalculationAnantha NarayananPas encore d'évaluation
- SY22-23+Annual+Report FinalDocument47 pagesSY22-23+Annual+Report FinalNorus LizaPas encore d'évaluation
- Oil List: Audi Front Axle DriveDocument35 pagesOil List: Audi Front Axle DriveAska QianPas encore d'évaluation
- PathologyDocument31 pagesPathologyStudy Usmle100% (1)
- 3) Uses and Gratification: 1) The Hypodermic Needle ModelDocument5 pages3) Uses and Gratification: 1) The Hypodermic Needle ModelMarikaMcCambridgePas encore d'évaluation
- Properties of WaterDocument23 pagesProperties of WaterNiken Rumani100% (1)
- Actron Vismin ReportDocument19 pagesActron Vismin ReportSirhc OyagPas encore d'évaluation
- Stratum CorneumDocument4 pagesStratum CorneumMuh Firdaus Ar-RappanyPas encore d'évaluation
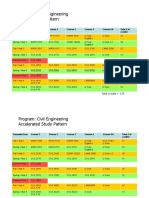
- HKUST 4Y Curriculum Diagram CIVLDocument4 pagesHKUST 4Y Curriculum Diagram CIVLfrevPas encore d'évaluation
- This Is A Short Presentation To Explain The Character of Uncle Sam, Made by Ivo BogoevskiDocument7 pagesThis Is A Short Presentation To Explain The Character of Uncle Sam, Made by Ivo BogoevskiIvo BogoevskiPas encore d'évaluation
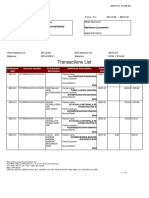
- Transactions List: Marilena Constantin RO75BRDE445SV93146784450 RON Marilena ConstantinDocument12 pagesTransactions List: Marilena Constantin RO75BRDE445SV93146784450 RON Marilena ConstantinConstantin MarilenaPas encore d'évaluation