Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Teorem Yds-Deneme-1 PDFDocument20 pagesTeorem Yds-Deneme-1 PDFyaseminbalimPas encore d'évaluation
- 11 Postnatal Care of The Mother and NewbornDocument15 pages11 Postnatal Care of The Mother and NewbornArabelle GO100% (1)
- Maternal Child Nursing: Dehydration, Hip Dysplasia, HydrocephalusDocument110 pagesMaternal Child Nursing: Dehydration, Hip Dysplasia, HydrocephalusVin Santos0% (1)
- Assessing The Nestle Boycott Corporate Accountability and Human Rights - Compressed-1-CompressedDocument19 pagesAssessing The Nestle Boycott Corporate Accountability and Human Rights - Compressed-1-CompressedCarla FrascaPas encore d'évaluation
- Hormonal Physiology of Childbearing All Fact SheetsDocument18 pagesHormonal Physiology of Childbearing All Fact SheetsFelix MolinaPas encore d'évaluation
- NP 1 To 5 Focus210-D WITHOUT AnswersDocument5 pagesNP 1 To 5 Focus210-D WITHOUT AnswersMarkie CubosPas encore d'évaluation
- Dextroamphetamine: Brand Name: DexedrineDocument23 pagesDextroamphetamine: Brand Name: DexedrineSharry Fe OasayPas encore d'évaluation
- Episode 127: Using The Dental Diet To Reverse Dental Problems With Dr. Steven LinDocument16 pagesEpisode 127: Using The Dental Diet To Reverse Dental Problems With Dr. Steven LinDianaVisanPas encore d'évaluation
- Essential Newborn Care ProtocolDocument23 pagesEssential Newborn Care ProtocolKaren Viviene CincoPas encore d'évaluation
- Awareness and Practice of Breast Feeding Among Mothers at Kiryandongo District HospitalDocument12 pagesAwareness and Practice of Breast Feeding Among Mothers at Kiryandongo District HospitalKIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- Ergonomics For ChildrenDocument27 pagesErgonomics For ChildrenRacquel CortezPas encore d'évaluation
- St. Paul University Community Health Nursing Work Plan and Action PlansDocument10 pagesSt. Paul University Community Health Nursing Work Plan and Action Plansimnas100% (1)
- Holy Family College of NursingDocument14 pagesHoly Family College of NursingSwati SharmaPas encore d'évaluation
- AFST 236 Final Paper - Discussing The Indiginous African Cultures of The Yoruba and IgboDocument17 pagesAFST 236 Final Paper - Discussing The Indiginous African Cultures of The Yoruba and IgboSierra HellemansPas encore d'évaluation
- Infant Formulas ExplainedDocument5 pagesInfant Formulas ExplainedDimitris TasiouPas encore d'évaluation
- MCN ReviewerDocument2 pagesMCN ReviewerJunghoon YangParkPas encore d'évaluation
- 7YTLP Year 1 Session 9 - Nutrition at Different Life Stage - From The Womb To Old AgeDocument20 pages7YTLP Year 1 Session 9 - Nutrition at Different Life Stage - From The Womb To Old Ageppnaawan2021100% (4)
- Iloilo City Regulation Ordinance 2014-526Document5 pagesIloilo City Regulation Ordinance 2014-526Iloilo City CouncilPas encore d'évaluation
- Summative AssessmentDocument11 pagesSummative AssessmentAzria John DemetriPas encore d'évaluation
- Understanding the Partograph for Monitoring LaborDocument14 pagesUnderstanding the Partograph for Monitoring Labornaomie manaliliPas encore d'évaluation
- 2015 Terminologi Asesmen FHDocument88 pages2015 Terminologi Asesmen FHPutri PuspitaPas encore d'évaluation
- Neonatal SepsisDocument8 pagesNeonatal Sepsis+nellaPas encore d'évaluation
- NCP Hydrocephalus With RationaleDocument42 pagesNCP Hydrocephalus With RationaleJulienne Sanchez-Salazar80% (15)
- Republic Act No. 9163 - : Week 1 - Lesson 1 Implementing NSTP Rules and RegulationsDocument13 pagesRepublic Act No. 9163 - : Week 1 - Lesson 1 Implementing NSTP Rules and RegulationsMary Ann F. MendezPas encore d'évaluation
- Natural Healing Through MacrobioticDocument189 pagesNatural Healing Through MacrobioticFady Nassar100% (9)
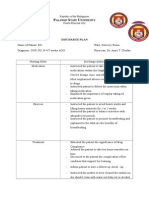
- Discharge Plan: Alawan Tate NiversityDocument2 pagesDischarge Plan: Alawan Tate NiversityLenieGracePascoPas encore d'évaluation
- Breast Engrogement FinalDocument41 pagesBreast Engrogement FinalSharmistha DebnathPas encore d'évaluation
- Understanding the Normal Puerperium ProcessDocument52 pagesUnderstanding the Normal Puerperium ProcessPiyush Dutta100% (1)
- Are Our Babies Off To A Healthy Start? The State of Implementation of The Global Strategy For Infant and Young Child Feeding in EuropeDocument12 pagesAre Our Babies Off To A Healthy Start? The State of Implementation of The Global Strategy For Infant and Young Child Feeding in EuropeSukma DewiPas encore d'évaluation
- Demonstration ON Care of Newborn PhototherapyDocument28 pagesDemonstration ON Care of Newborn PhototherapyA J Fathima100% (1)