Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Penyakit DegeneratifDocument29 pagesPenyakit DegeneratifMuhammad Rizki RamadanaPas encore d'évaluation
- Bksap Vacant 2018 eDocument65 pagesBksap Vacant 2018 eMuhammad Rizki RamadanaPas encore d'évaluation
- 3 BAB 2sDocument26 pages3 BAB 2sMuhammad Rizki RamadanaPas encore d'évaluation
- Stevens-Johnson Syndrome: Case ReportDocument1 pageStevens-Johnson Syndrome: Case ReportMuhammad Rizki RamadanaPas encore d'évaluation
- 19 01Document4 pages19 01Muhammad Rizki RamadanaPas encore d'évaluation
- Cerebral Palsy An Overview 2018Document11 pagesCerebral Palsy An Overview 2018Yhuliana AcostaPas encore d'évaluation
- Enzymes - What The Experts KnowDocument252 pagesEnzymes - What The Experts KnowRocio Uresti De Ramirez0% (1)
- Nash Leaders in TyphoidDocument25 pagesNash Leaders in TyphoidhompatPas encore d'évaluation
- Hepatitis BDocument61 pagesHepatitis BMichael AmandyPas encore d'évaluation
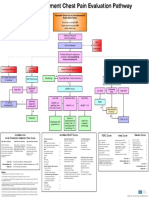
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidPas encore d'évaluation
- 21st Century DiseasesDocument8 pages21st Century DiseasesPapanaga ArinaPas encore d'évaluation
- Biliary Tract DiseaseDocument52 pagesBiliary Tract DiseaseAna Cotoman100% (1)
- Sexual HealthDocument11 pagesSexual Healthapi-236516264Pas encore d'évaluation
- Pathology MCQsDocument10 pagesPathology MCQsAnuradha Nanayakkara0% (2)
- Organic DiseasesDocument3 pagesOrganic DiseasesGlenn Cabance LelinaPas encore d'évaluation
- Modal & Phrasal VerbsDocument5 pagesModal & Phrasal VerbsPaf VenancioPas encore d'évaluation
- Algoritma CKD PDFDocument2 pagesAlgoritma CKD PDFDesla Citra100% (1)
- Typhoid FeverDocument11 pagesTyphoid FeverjhenvitoPas encore d'évaluation
- ExcerptDocument2 pagesExcerptcoloPas encore d'évaluation
- Biers BlockDocument4 pagesBiers Blockemkay1234Pas encore d'évaluation
- The Well Known Metal - Aurum Met PersonalityDocument81 pagesThe Well Known Metal - Aurum Met PersonalityDr. Deepthi BS100% (1)
- Sea RemediesDocument2 pagesSea Remedieskaravi schiniasPas encore d'évaluation
- Measles (Case Presentation)Document19 pagesMeasles (Case Presentation)Zam Pamate100% (3)
- Asthma or Copd Case StudyDocument10 pagesAsthma or Copd Case StudyMahendra ShrimaliPas encore d'évaluation
- Paragraph DevelopmentDocument7 pagesParagraph DevelopmentJacqueline Gregorio RamosPas encore d'évaluation
- Nutri Lec ReviewerDocument182 pagesNutri Lec ReviewerRaquel MonsalvePas encore d'évaluation
- Case PresentationDocument14 pagesCase PresentationFatema RavatPas encore d'évaluation
- Health FceDocument5 pagesHealth FceDoru AndreiPas encore d'évaluation
- Geriatric NursingDocument64 pagesGeriatric NursingMark Elben100% (2)
- Dengue, Chikungunya Yellow Fever: Dr. Saida SharminDocument48 pagesDengue, Chikungunya Yellow Fever: Dr. Saida SharminBishwajit BhattacharjeePas encore d'évaluation
- 02-09 2022 Pharm Pediatrics 2022 R4Document44 pages02-09 2022 Pharm Pediatrics 2022 R4Amira HelayelPas encore d'évaluation
- Awareness Knowledge and Attitude About Dengue AmonDocument5 pagesAwareness Knowledge and Attitude About Dengue AmonSachintha PasinduPas encore d'évaluation
- Neurological Disease in Lupus: Toward A Personalized Medicine ApproachDocument12 pagesNeurological Disease in Lupus: Toward A Personalized Medicine ApproachjerejerejerePas encore d'évaluation
- 4 Stool Culture PDFDocument35 pages4 Stool Culture PDFVenny PatriciaPas encore d'évaluation
- QuestionsDocument6 pagesQuestionsLorvic Andrew Juanson UmaliPas encore d'évaluation