Vous aimerez peut-être aussi
- East Meets West: Chinese Chi Healing for Western Sexual DisordersD'EverandEast Meets West: Chinese Chi Healing for Western Sexual DisordersPas encore d'évaluation
- Evidence-based Therapy of Psoriasis: Focus on BiologicsD'EverandEvidence-based Therapy of Psoriasis: Focus on BiologicsPas encore d'évaluation
- Yoga, Meditation and Mindfulness Ultimate Guide: 3 Books In 1 Boxed Set - Perfect for Beginners with Yoga Poses: 3 Books In 1 Boxed Set - Perfect for Beginners with Yoga PosesD'EverandYoga, Meditation and Mindfulness Ultimate Guide: 3 Books In 1 Boxed Set - Perfect for Beginners with Yoga Poses: 3 Books In 1 Boxed Set - Perfect for Beginners with Yoga PosesPas encore d'évaluation
- Convergence of Consciousness The Harmonics of Creation: with Study GuideD'EverandConvergence of Consciousness The Harmonics of Creation: with Study GuideÉvaluation : 1 sur 5 étoiles1/5 (1)
- Pregnancy Made Comfortable - with Yoga & Dietetics: A Complete reference book covering all the stages from pre-pregnancy to post-pregnancyD'EverandPregnancy Made Comfortable - with Yoga & Dietetics: A Complete reference book covering all the stages from pre-pregnancy to post-pregnancyPas encore d'évaluation
- Teaching Yoga and Meditation Beyond the Poses: An unique and practical workbookD'EverandTeaching Yoga and Meditation Beyond the Poses: An unique and practical workbookPas encore d'évaluation
- Live. Learn. Grow.: A Spiritual and Personal Growth JourneyD'EverandLive. Learn. Grow.: A Spiritual and Personal Growth JourneyPas encore d'évaluation
- Into the Heart of Health: Reaching Your Health Threshold, an Unshakeable Balance in Mind, Body, and EmotionsD'EverandInto the Heart of Health: Reaching Your Health Threshold, an Unshakeable Balance in Mind, Body, and EmotionsPas encore d'évaluation
- Diaphragm Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandDiaphragm Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Meditation and Yoga in Psychotherapy: Techniques for Clinical PracticeD'EverandMeditation and Yoga in Psychotherapy: Techniques for Clinical PracticePas encore d'évaluation
- Holistic Postpartum Manual: Maternal Health Manuals, #3D'EverandHolistic Postpartum Manual: Maternal Health Manuals, #3Pas encore d'évaluation
- STRESS MANAGEMENT FOR WOMEN: From chaos to harmony - Create a good flow in your work and relationshipD'EverandSTRESS MANAGEMENT FOR WOMEN: From chaos to harmony - Create a good flow in your work and relationshipPas encore d'évaluation
- Of Bubbles, Buddha, and Butterflies: How This Butterfly Found Her Wings Without Leaving the GroundD'EverandOf Bubbles, Buddha, and Butterflies: How This Butterfly Found Her Wings Without Leaving the GroundPas encore d'évaluation
- A Beginners Approach to Unseen Reality or Drops in the OceanD'EverandA Beginners Approach to Unseen Reality or Drops in the OceanPas encore d'évaluation
- Hallux Varus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandHallux Varus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- From Havoc to Harmony: 5 Steps to Restore Peace at Home and Rebuild Your Relationship with Your Adhd ChildD'EverandFrom Havoc to Harmony: 5 Steps to Restore Peace at Home and Rebuild Your Relationship with Your Adhd ChildPas encore d'évaluation
- Principles of Healing Through Movement: An Alternative Holistic Approach to Therapeutic Movement for those with Cancer and/or Chronic IllnessD'EverandPrinciples of Healing Through Movement: An Alternative Holistic Approach to Therapeutic Movement for those with Cancer and/or Chronic IllnessPas encore d'évaluation
- From Alignment to Enlightenment: The Path to Joy and PeaceD'EverandFrom Alignment to Enlightenment: The Path to Joy and PeacePas encore d'évaluation
- Journey Through PTSD: Navigating Healing and HopeD'EverandJourney Through PTSD: Navigating Healing and HopeÉvaluation : 5 sur 5 étoiles5/5 (1)
- Exercise For Mood: Move For Happy - Discover How Simple Workout Plant Can Increase Emotional Regulation, Release Hormones To Lift Mood, and Keep You FitD'EverandExercise For Mood: Move For Happy - Discover How Simple Workout Plant Can Increase Emotional Regulation, Release Hormones To Lift Mood, and Keep You FitPas encore d'évaluation
- Reconnecting to Self-Healing: The Art of Advocating for YourselfD'EverandReconnecting to Self-Healing: The Art of Advocating for YourselfPas encore d'évaluation
- Our Unconscious Mind and How to Use It (Barnes & Noble Digital Library)D'EverandOur Unconscious Mind and How to Use It (Barnes & Noble Digital Library)Pas encore d'évaluation
- Enhancing the Benefits of Nauli with a Key Exercise for Abdominal Muscle StrengthD'EverandEnhancing the Benefits of Nauli with a Key Exercise for Abdominal Muscle StrengthÉvaluation : 5 sur 5 étoiles5/5 (1)
- The Journey to Pain Relief: A Hands-On Guide to Breakthroughs in Pain TreatmentD'EverandThe Journey to Pain Relief: A Hands-On Guide to Breakthroughs in Pain TreatmentÉvaluation : 4.5 sur 5 étoiles4.5/5 (3)
- Finding Grace and Balance in the Cycle of Life: Exploring Integrative GynecologyD'EverandFinding Grace and Balance in the Cycle of Life: Exploring Integrative GynecologyPas encore d'évaluation
- The Qi of Taking a Medical History and Performing a Physical ExaminationD'EverandThe Qi of Taking a Medical History and Performing a Physical ExaminationPas encore d'évaluation
- Relaxation and Stress Reduction for Beginners: A Mindfulness-Based ProgramD'EverandRelaxation and Stress Reduction for Beginners: A Mindfulness-Based ProgramPas encore d'évaluation
- Sit With Less Pain: Gentle Yoga for Meditators and Everyone ElseD'EverandSit With Less Pain: Gentle Yoga for Meditators and Everyone ElsePas encore d'évaluation
- Life, Nutrition, and Wellness 101: A Holistic Approach with a Philosophical TwistD'EverandLife, Nutrition, and Wellness 101: A Holistic Approach with a Philosophical TwistPas encore d'évaluation
- TENDER PEACE: Moon, Tree and Flower Meditations for Pregnancy and BeyondD'EverandTENDER PEACE: Moon, Tree and Flower Meditations for Pregnancy and BeyondPas encore d'évaluation
- Meditation for Motherhood: Zen Meditation for Conception, Pregnancy, and BirthD'EverandMeditation for Motherhood: Zen Meditation for Conception, Pregnancy, and BirthPas encore d'évaluation
- A Simple Guide to Slouching Posture, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Slouching Posture, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- More Than A Treatment: How To Create Exceptional Experiences That Increase Patient Satisfaction AnD'EverandMore Than A Treatment: How To Create Exceptional Experiences That Increase Patient Satisfaction AnPas encore d'évaluation
- Hazing Aging: How Capillary Endothelia Control Inflammation and AgingD'EverandHazing Aging: How Capillary Endothelia Control Inflammation and AgingPas encore d'évaluation
- Before SEVEN-THIRTY: Practical Ways to Empower Yourself and Save YOUR Relationship Before Giving UpD'EverandBefore SEVEN-THIRTY: Practical Ways to Empower Yourself and Save YOUR Relationship Before Giving UpPas encore d'évaluation
- Vagus Nerve, Vagal Tone & Polyvagal Theory: Activate Your Natural Healing Power to Reduce Depression, Anxiety and StressD'EverandVagus Nerve, Vagal Tone & Polyvagal Theory: Activate Your Natural Healing Power to Reduce Depression, Anxiety and StressPas encore d'évaluation
- Boost Getting Pregnant: Surprisingly Simple Natural Ways To Remedy InfertilityD'EverandBoost Getting Pregnant: Surprisingly Simple Natural Ways To Remedy InfertilityPas encore d'évaluation
- Health at Home: Sustainable and Healthy Building and LivingD'EverandHealth at Home: Sustainable and Healthy Building and LivingPas encore d'évaluation
- The Divine SelfQare Strategy: A Wellness Guide To Total Body AlignmentD'EverandThe Divine SelfQare Strategy: A Wellness Guide To Total Body AlignmentPas encore d'évaluation
- Soul Doctoring: Heal Yourself, Heal the PlanetD'EverandSoul Doctoring: Heal Yourself, Heal the PlanetPas encore d'évaluation
- Pain Pathways & Pain ManagementDocument82 pagesPain Pathways & Pain ManagementAarthiPas encore d'évaluation
- Shaukat Khanum Memorial Cancer Hospital & Research CentreDocument2 pagesShaukat Khanum Memorial Cancer Hospital & Research CentreUsama AjmalPas encore d'évaluation
- Uterine FibroidsDocument46 pagesUterine FibroidsRavindranatha AnPas encore d'évaluation
- Uterine Fibroids: Q: What Are Fibroids? ADocument8 pagesUterine Fibroids: Q: What Are Fibroids? Abasantjain12345Pas encore d'évaluation
- Lap Ok HisterektomiDocument4 pagesLap Ok HisterektomiHappy Martha NababanPas encore d'évaluation
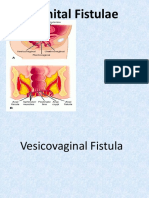
- Fistula GenitaliaDocument35 pagesFistula GenitaliaFifi FruitasariPas encore d'évaluation
- Abdominal HysterectomyDocument23 pagesAbdominal Hysterectomytata marethaPas encore d'évaluation
- Copy3-Obgyn Final Base LvivtechDocument3 466 pagesCopy3-Obgyn Final Base LvivtechHart ElettPas encore d'évaluation
- Total Laparo Hysterectomy TLHDocument4 pagesTotal Laparo Hysterectomy TLHSujoyDePas encore d'évaluation
- CGHS Rates for Medical Procedures in BangaloreDocument23 pagesCGHS Rates for Medical Procedures in BangaloreVasu RathodPas encore d'évaluation
- 2021 Fibroid Uterus Surgical Challenges inDocument200 pages2021 Fibroid Uterus Surgical Challenges inHAVIZ YUADPas encore d'évaluation
- Rguhs ObgDocument29 pagesRguhs ObgKabilesh SelvarajPas encore d'évaluation
- Cesarean Section PatelDocument55 pagesCesarean Section Patelالوافي الذهبيPas encore d'évaluation
- Esquivel ComplaintDocument18 pagesEsquivel ComplaintStatesman JournalPas encore d'évaluation
- Menorrhagia and Management PDFDocument4 pagesMenorrhagia and Management PDFrizkyPas encore d'évaluation
- 50 Studies Every Obstetrician-Gynecologist Should Know 1Document70 pages50 Studies Every Obstetrician-Gynecologist Should Know 1Deepak Sugumar100% (2)
- Obs & Gynae InstrumentsDocument66 pagesObs & Gynae InstrumentsEng AbdiRahim Khalif Ali71% (7)
- 3Document8 pages3Agung SentosaPas encore d'évaluation
- HysterectomyDocument10 pagesHysterectomyjhodanePas encore d'évaluation
- Abnormal Vaginal Bleeding Policar 051611Document69 pagesAbnormal Vaginal Bleeding Policar 051611bidan22Pas encore d'évaluation
- Understanding Uterine FibroidsDocument2 pagesUnderstanding Uterine FibroidsSahaaneiy IlmeePas encore d'évaluation
- Committee To Review The Health Effects in Vietnam Veterans of Exposure To Herbicides (Ninth Biennial Update)Document34 pagesCommittee To Review The Health Effects in Vietnam Veterans of Exposure To Herbicides (Ninth Biennial Update)Children Of Vietnam Veterans Health Alliance100% (1)
- Makalah Rule of Ultrasound in Management of Uterine LeiomyomaDocument23 pagesMakalah Rule of Ultrasound in Management of Uterine LeiomyomaKristabella GianinaPas encore d'évaluation
- Total Abdominal Hysterectomy and Bilateral Salpingo-Oophorectomy Procedure OutlineDocument6 pagesTotal Abdominal Hysterectomy and Bilateral Salpingo-Oophorectomy Procedure OutlineMyraPas encore d'évaluation
- Ectopic Pregnancy H Mole Posted Jan 10 2024Document10 pagesEctopic Pregnancy H Mole Posted Jan 10 2024hsgarolacanPas encore d'évaluation
- Guidelines For Distt Hospitals - Indian Public Health StandardsDocument124 pagesGuidelines For Distt Hospitals - Indian Public Health StandardsTejinder SinghPas encore d'évaluation
- Rare Case of Pelvic Schwannoma Mimicking Intra-Ligamenter Uterine Fibroid A Case ReportDocument5 pagesRare Case of Pelvic Schwannoma Mimicking Intra-Ligamenter Uterine Fibroid A Case ReportSatrya WibawaPas encore d'évaluation
- Uterine MyomaDocument45 pagesUterine MyomaAndiniMayudhaPas encore d'évaluation
- The Modified Radical Peripartum Cesarean Hysterectomy (Soleymani-Alazzam-Collins Technique) - A Systematic, Safe Procedure For The Management of Severe Placenta Accreta SpectrumDocument10 pagesThe Modified Radical Peripartum Cesarean Hysterectomy (Soleymani-Alazzam-Collins Technique) - A Systematic, Safe Procedure For The Management of Severe Placenta Accreta SpectrumSaira MendozaPas encore d'évaluation
- Test 3 4 5Document8 pagesTest 3 4 5Sayani BanerjeePas encore d'évaluation
- B Lynch SuturingDocument32 pagesB Lynch SuturingDoru Draghici67% (3)