Vous aimerez peut-être aussi
- Client Consultation CardDocument3 pagesClient Consultation Cardapi-614534740100% (1)
- Medical FormDocument4 pagesMedical FormSujata DeviPas encore d'évaluation
- FOH-25 Tuberculosis Screening (M.25)Document1 pageFOH-25 Tuberculosis Screening (M.25)Maria CabañasPas encore d'évaluation
- Pre-Employment Medical ExaminationDocument4 pagesPre-Employment Medical ExaminationRohit Chaudhary100% (1)
- Medical CertificateDocument1 pageMedical CertificateArgie Joy Marie AmpolPas encore d'évaluation
- Pre-participation Physical Evaluation HISTORY and PHYSICAL EXAM FormsDocument2 pagesPre-participation Physical Evaluation HISTORY and PHYSICAL EXAM FormsCindy Hayes ShultzPas encore d'évaluation
- Chest XDocument8 pagesChest XAnnandra RahmanPas encore d'évaluation
- HACCP Thermometer Calibration Log - Maintain Food SafetyDocument1 pageHACCP Thermometer Calibration Log - Maintain Food SafetyArman Al NasarPas encore d'évaluation
- HPV Vaccine Powerpoint PresentationDocument18 pagesHPV Vaccine Powerpoint Presentationkristia destiPas encore d'évaluation
- OTHM-HEALTH AND SAFETY MANAGEMENT PRINCIPLES AND POLICY - Unit 01Document3 pagesOTHM-HEALTH AND SAFETY MANAGEMENT PRINCIPLES AND POLICY - Unit 01dinesh manikantaPas encore d'évaluation
- Medical exam form summaryDocument4 pagesMedical exam form summaryAldwin Bagtas0% (1)
- Medical Certificate Template 12Document1 pageMedical Certificate Template 12K.O.R. Gaming100% (1)
- Pre-Employment Medical FormsDocument8 pagesPre-Employment Medical Formsnot your medz duranPas encore d'évaluation
- HPCL medical standardsDocument5 pagesHPCL medical standardsConceptual GATE & ESEPas encore d'évaluation
- RivasnicuDocument3 pagesRivasnicuapi-613460741Pas encore d'évaluation
- History Form: Reparticipation Hysical ValuationDocument4 pagesHistory Form: Reparticipation Hysical ValuationHariPas encore d'évaluation
- Pre-Employment Guiding PrinciplesDocument14 pagesPre-Employment Guiding PrinciplesVivek SPas encore d'évaluation
- Random Drug Test: CertificationDocument2 pagesRandom Drug Test: CertificationApril BoreresPas encore d'évaluation
- Summer Study at The University of Colorado BoulderDocument1 pageSummer Study at The University of Colorado BoulderJan MarcPas encore d'évaluation
- Pre Medical Evaluatiom Form PFT 1 PDFDocument2 pagesPre Medical Evaluatiom Form PFT 1 PDFAIEN WENDELEIH Q. CAPINPIN100% (1)
- Scat3: Sport Concussion Assessment Tool - 3rd EditionDocument4 pagesScat3: Sport Concussion Assessment Tool - 3rd EditionPhil ThomsonPas encore d'évaluation
- Daily Repositioning Skin Inspection ChartDocument2 pagesDaily Repositioning Skin Inspection Chartsafasayed100% (1)
- Medical History QuestionnaireDocument3 pagesMedical History QuestionnaireIrene IonescuPas encore d'évaluation
- COVID 19 Positive Test Report Form: 24 HoursDocument2 pagesCOVID 19 Positive Test Report Form: 24 HoursRaju SambhePas encore d'évaluation
- Drug Test Request FormDocument6 pagesDrug Test Request FormOptimaCare MalabonPas encore d'évaluation
- IIMU MBA 2020 A8 Medical Fitness CertificateDocument1 pageIIMU MBA 2020 A8 Medical Fitness CertificateAayoush GuptaPas encore d'évaluation
- Hygeia Lifestyle Intake QuestionnaireDocument6 pagesHygeia Lifestyle Intake QuestionnaireVivek GuptaPas encore d'évaluation
- Pocedure ConsentDocument2 pagesPocedure ConsentJack TedescoPas encore d'évaluation
- MediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Document2 pagesMediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Lhogeswaran RaviPas encore d'évaluation
- Fitness For Work PolicyDocument2 pagesFitness For Work Policyjaultry muhuyiPas encore d'évaluation
- Claim by Nominee, Department of Post, IndiaDocument1 pageClaim by Nominee, Department of Post, IndiaSondeep Ahuja70% (10)
- Florida A&M University Athletic Pre-Participation HistoryDocument3 pagesFlorida A&M University Athletic Pre-Participation HistorydraykidPas encore d'évaluation
- HOPE 1 Aerobics FinalDocument30 pagesHOPE 1 Aerobics FinalBruce GonzalvoPas encore d'évaluation
- Baseline Occupational Medical Evaluation Proposed Reporting Revised FormatDocument3 pagesBaseline Occupational Medical Evaluation Proposed Reporting Revised FormatAhmed OsmanPas encore d'évaluation
- Occupational Health FormDocument3 pagesOccupational Health FormCherry Mañibo100% (1)
- Short Employee Service AssessmentDocument2 pagesShort Employee Service Assessmentdennisjuntak100% (1)
- Cascadian Building Monthly Safety Meeting AgendaDocument1 pageCascadian Building Monthly Safety Meeting AgendaRAZALIKARIMPas encore d'évaluation
- Hiv Aids 7 Hour Training CertDocument1 pageHiv Aids 7 Hour Training Certapi-472652222Pas encore d'évaluation
- Unit Ig1: Management of Health and SafetyDocument15 pagesUnit Ig1: Management of Health and SafetyVikash Kumar RayPas encore d'évaluation
- Screening for High Blood Sugar Saves LivesDocument4 pagesScreening for High Blood Sugar Saves LivesRevalitha PutriPas encore d'évaluation
- Nursing Assessment ToolDocument6 pagesNursing Assessment ToolRaniPas encore d'évaluation
- Physical fitness certificateDocument1 pagePhysical fitness certificateEluri Mahesh NaniPas encore d'évaluation
- Final Customer FeedbackDocument2 pagesFinal Customer FeedbackRohit KaliaPas encore d'évaluation
- 01 Nursing Note SampleDocument1 page01 Nursing Note Sampletesttest testPas encore d'évaluation
- AIA Singapore Health Declaration FormDocument4 pagesAIA Singapore Health Declaration FormkotisanampudiPas encore d'évaluation
- STD Symptoms, Tests, and Treatments ExplainedDocument19 pagesSTD Symptoms, Tests, and Treatments ExplainedJayvah EstrellaPas encore d'évaluation
- Medical History and Evaluation FormDocument22 pagesMedical History and Evaluation FormJobelle Fernandez-SantosPas encore d'évaluation
- Employees Accedent ReportDocument1 pageEmployees Accedent ReportKomal TiwariPas encore d'évaluation
- Blood Requisition FormDocument2 pagesBlood Requisition FormPrashant Kumar Singh100% (1)
- Sample Accident Report FormDocument1 pageSample Accident Report FormKrishna SrikanthPas encore d'évaluation
- Attending Physicians Statement-Disability Claim Ver2.1 - English - tcm47-27477Document2 pagesAttending Physicians Statement-Disability Claim Ver2.1 - English - tcm47-27477saika tabbasumPas encore d'évaluation
- General Assessment TemplateDocument8 pagesGeneral Assessment TemplateBob HopePas encore d'évaluation
- General Medical History Form PDFDocument1 pageGeneral Medical History Form PDFണг. ധн¡тε H̶A̶T̶Pas encore d'évaluation
- Reliance Health Insurance Pre Authorisation FormDocument4 pagesReliance Health Insurance Pre Authorisation FormM/s MicrotechPas encore d'évaluation
- Medical and dental referral formsDocument2 pagesMedical and dental referral formsMark Darvin BucoyPas encore d'évaluation
- Hospital Training CertificateDocument1 pageHospital Training CertificateSapna KumariPas encore d'évaluation
- Workplace Injury Report FormDocument3 pagesWorkplace Injury Report FormMani VannanPas encore d'évaluation
- Health Related Fitness Assessments Turning This in PDFDocument3 pagesHealth Related Fitness Assessments Turning This in PDFRyan loudPas encore d'évaluation
- Patient Registration Form: General Information (Please Print Neatly)Document5 pagesPatient Registration Form: General Information (Please Print Neatly)Dan ThomasPas encore d'évaluation
- Apply European Training ServicesDocument2 pagesApply European Training ServicesDobrin Tina IasminaPas encore d'évaluation
- MP 010 Rev 002 Duck R Manual Ingles Uk 03 02 2021 Prod PDF - 1643901641Document2 pagesMP 010 Rev 002 Duck R Manual Ingles Uk 03 02 2021 Prod PDF - 1643901641RasLDKPas encore d'évaluation
- Fact Sheets: Working Safely Around Radiofrequency (RF) TransmittersDocument8 pagesFact Sheets: Working Safely Around Radiofrequency (RF) TransmittersRasLDKPas encore d'évaluation
- Rescue Plan: Fall Protection ProgramDocument6 pagesRescue Plan: Fall Protection ProgramTFattah100% (2)
- Technical Notice Avao Bod Bod Fast Ce 2Document2 pagesTechnical Notice Avao Bod Bod Fast Ce 2RasLDKPas encore d'évaluation
- Technical Notice ASCENSION 4Document16 pagesTechnical Notice ASCENSION 4internetPas encore d'évaluation
- A Guide To Radio Frequency Hazards With Electric DetonatorsDocument26 pagesA Guide To Radio Frequency Hazards With Electric Detonatorsarmeidian dannyPas encore d'évaluation
- OSHA Tower Fall Prevention Training MaterialsDocument74 pagesOSHA Tower Fall Prevention Training MaterialsRasLDKPas encore d'évaluation
- Tower Climbing ProcedureDocument33 pagesTower Climbing ProcedurePyara Kamboj50% (2)
- Technical Notice ASAP LOCK CE 1Document26 pagesTechnical Notice ASAP LOCK CE 1RasLDKPas encore d'évaluation
- Tower Manual: COMDTINST M11000.4A JANUARY 2002Document214 pagesTower Manual: COMDTINST M11000.4A JANUARY 2002adnan100% (3)
- Descendedor IdDocument29 pagesDescendedor IdNathaly Moreno RodríguezPas encore d'évaluation
- A Guide To Radio Frequency Hazards With Electric DetonatorsDocument26 pagesA Guide To Radio Frequency Hazards With Electric Detonatorsarmeidian dannyPas encore d'évaluation
- Emergency Response PlanningDocument8 pagesEmergency Response Planningjr_mcmillinPas encore d'évaluation
- Authorized Tower Climber and Rescue: Course DescriptionDocument5 pagesAuthorized Tower Climber and Rescue: Course DescriptionRasLDKPas encore d'évaluation
- Tower Manual: COMDTINST M11000.4A JANUARY 2002Document214 pagesTower Manual: COMDTINST M11000.4A JANUARY 2002RasLDKPas encore d'évaluation
- D-Lux 5 Brochure - enDocument15 pagesD-Lux 5 Brochure - encalajavaPas encore d'évaluation
- Syllabus Industry Tools, Tower Climbing and Rescue ENER-1020Document11 pagesSyllabus Industry Tools, Tower Climbing and Rescue ENER-1020RasLDKPas encore d'évaluation
- Fall Protection For Telecom TowersDocument8 pagesFall Protection For Telecom TowersRasLDKPas encore d'évaluation
- Fall Protection For Telecom TowersDocument8 pagesFall Protection For Telecom TowersRasLDKPas encore d'évaluation
- 400 TowerConstruction SillimanDavies BO2 FinalDocument185 pages400 TowerConstruction SillimanDavies BO2 FinalAnonymous JcgSiw2jMbPas encore d'évaluation
- Vertical Access BrochureDocument20 pagesVertical Access BrochureRasLDKPas encore d'évaluation
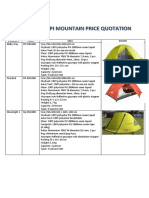
- Merapi - Mountain - Price Quotation PDFDocument3 pagesMerapi - Mountain - Price Quotation PDFRandy Prabha YoganaPas encore d'évaluation
- Syllabus For Irata Level 1 Rope Access TechnicianDocument3 pagesSyllabus For Irata Level 1 Rope Access TechnicianRasLDKPas encore d'évaluation
- Risk Assessment Method Statement FocusDocument4 pagesRisk Assessment Method Statement FocusRasLDKPas encore d'évaluation
- ASAP Detailed PDFDocument19 pagesASAP Detailed PDFRasLDKPas encore d'évaluation
- Syllabus For Irata Level 1 Rope Access TechnicianDocument3 pagesSyllabus For Irata Level 1 Rope Access TechnicianRasLDKPas encore d'évaluation
- Workplace Learning Logbook Templates PDFDocument4 pagesWorkplace Learning Logbook Templates PDFRasLDKPas encore d'évaluation
- Syllabus For Irata Level 1 Rope Access TechnicianDocument3 pagesSyllabus For Irata Level 1 Rope Access TechnicianRasLDKPas encore d'évaluation
- MILLET Expedition Project 2015 RulesDocument9 pagesMILLET Expedition Project 2015 RulesRasLDKPas encore d'évaluation
- Fall ClearanceDocument1 pageFall ClearanceRasLDKPas encore d'évaluation
- Hiv V/S Aids: Other Differences Between HIV and AIDS Are Mentioned Below: HIV Is A Virus ThatDocument1 pageHiv V/S Aids: Other Differences Between HIV and AIDS Are Mentioned Below: HIV Is A Virus ThatTanya Gupta Srivastava100% (1)
- Drug Study Form 1Document7 pagesDrug Study Form 1Allyssa HeartPas encore d'évaluation
- Hyperthyroidism of The Child in Abidjan Cote Divoire Retrospective Study of 27 CaseDocument5 pagesHyperthyroidism of The Child in Abidjan Cote Divoire Retrospective Study of 27 CaseArif Rahman FarisPas encore d'évaluation
- 1 BellsPalsy PDFDocument14 pages1 BellsPalsy PDFSimbakutty VenkataramananPas encore d'évaluation
- VDRL/RPR: Dominic Edward Z. TomasDocument26 pagesVDRL/RPR: Dominic Edward Z. TomasDominic TomasPas encore d'évaluation
- Odd and CDDocument29 pagesOdd and CDRiyaSinghPas encore d'évaluation
- Rano BMDocument9 pagesRano BMMaria Claudia Rodriguez ZavaletaPas encore d'évaluation
- Book Let Shama Sharma Research EditDocument18 pagesBook Let Shama Sharma Research Editsai projectPas encore d'évaluation
- Generalized LymphadenopathyDocument20 pagesGeneralized LymphadenopathyBhabuk GhmPas encore d'évaluation
- Nursing Care Plan for Syphilis TreatmentDocument4 pagesNursing Care Plan for Syphilis Treatmentblaire100% (1)
- Artritis ReumatoideDocument73 pagesArtritis ReumatoideCastillo DiegoPas encore d'évaluation
- Stool Exam HandoutDocument5 pagesStool Exam HandoutAhmed GaberPas encore d'évaluation
- Disfuncion Erectil y Farmacos.Document7 pagesDisfuncion Erectil y Farmacos.Danisse RoaPas encore d'évaluation
- Retinopathy of PrematurityDocument7 pagesRetinopathy of PrematurityDewi PermatasariPas encore d'évaluation
- Guide to the intercollegiate MRCS (ENT) examDocument18 pagesGuide to the intercollegiate MRCS (ENT) exammonirul islam shohanPas encore d'évaluation
- Garrahy 2020Document13 pagesGarrahy 2020Ana Elizabeth Gangotena CoralPas encore d'évaluation
- Hepatitis Tests DiagnosisDocument2 pagesHepatitis Tests DiagnosisSyed FlyntPas encore d'évaluation
- Anesthetic Consideration For Neuromuscular DiseasesDocument6 pagesAnesthetic Consideration For Neuromuscular DiseasesALEJANDRO BOTERO FERNANDEZPas encore d'évaluation
- Vaginal Hysterectomy GuideDocument5 pagesVaginal Hysterectomy Guidesensitivity23Pas encore d'évaluation
- Common Causes and Management of Pediatric Convulsive Status EpilepticusDocument7 pagesCommon Causes and Management of Pediatric Convulsive Status EpilepticusAlberto VictorPas encore d'évaluation
- Pyometra in Small Animals - Reproductive System - Veterinary Manual PDFDocument3 pagesPyometra in Small Animals - Reproductive System - Veterinary Manual PDFKirti JamwalPas encore d'évaluation
- JurnalDocument5 pagesJurnalQorin Diin ArifniPas encore d'évaluation
- Cas 14835Document12 pagesCas 14835Sediki ZakariaPas encore d'évaluation
- Learners With Intellectual DisabilityDocument25 pagesLearners With Intellectual DisabilityCharine Blaza CorpuzPas encore d'évaluation
- Physiology Assignment: Complete Blood CountDocument7 pagesPhysiology Assignment: Complete Blood CountMuhammad ShahbazPas encore d'évaluation
- Clinical Manifestations and Treatment of Osteoporotic Thoracolumbar Vertebral Compression FracturesDocument19 pagesClinical Manifestations and Treatment of Osteoporotic Thoracolumbar Vertebral Compression Fracturesmnunezh2304Pas encore d'évaluation
- Introduction To PathophysiologyDocument3 pagesIntroduction To PathophysiologyНадежда КравченкоPas encore d'évaluation
- Tuberculosis: WHO Global Tuberculosis Report 2014Document2 pagesTuberculosis: WHO Global Tuberculosis Report 2014blueicelandPas encore d'évaluation
- Mapeh 9 - HealthDocument5 pagesMapeh 9 - HealthBeyoung GamefightPas encore d'évaluation
- NCP - Cellular AberrationDocument1 pageNCP - Cellular Aberrationissaiahnicolle100% (1)