Vous aimerez peut-être aussi
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Esearch Aper: Send The Reserve! New Ways To Support NATO Through Reserve ForcesDocument12 pagesEsearch Aper: Send The Reserve! New Ways To Support NATO Through Reserve ForcesIntruso2Pas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- PYNG FAST Analisis de Eficacia Del SistemaDocument7 pagesPYNG FAST Analisis de Eficacia Del SistemaIntruso2Pas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Kragh Ann SurgDocument7 pagesKragh Ann SurgIntruso2Pas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Practice: Teaching Case ReportDocument4 pagesPractice: Teaching Case ReportIntruso2Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- KING DAVID Historical CommentaryDocument21 pagesKING DAVID Historical CommentaryAndy NunezPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Battle of StalingradDocument11 pagesThe Battle of StalingradСтефан Трајковиќ100% (1)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Midland Publishing - US Air Force - The New CenturyDocument176 pagesMidland Publishing - US Air Force - The New CenturyNickiedeposiePas encore d'évaluation
- Packaging - MB Trousers LabelsDocument7 pagesPackaging - MB Trousers LabelsSiva KumarPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- India-China Conflict: Why in NewsDocument7 pagesIndia-China Conflict: Why in NewsMahesh JhaPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- JSMDQTFRDocument285 pagesJSMDQTFRBiblioteca ICEL Cuautitlán IzcalliPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
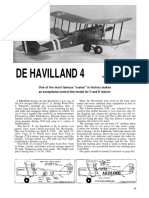
- De Havilland DH4Document3 pagesDe Havilland DH4RosanaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Subhash Chandra BoseDocument2 pagesSubhash Chandra BoseShubham KumarPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Order of The TempleDocument7 pagesOrder of The Templeamatorob7017Pas encore d'évaluation
- TYPE-MOON Character Material PDFDocument75 pagesTYPE-MOON Character Material PDFSander CCPas encore d'évaluation
- Does Factionalization of Insurgents Matter?: ACADEMIA LettersDocument5 pagesDoes Factionalization of Insurgents Matter?: ACADEMIA LettersAdedayo MichaelPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Cvsu Silang Rotc Unit Individual Progress Chart Sy: 2018 - 2019Document21 pagesCvsu Silang Rotc Unit Individual Progress Chart Sy: 2018 - 2019Chester CuarentasPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Liflet Ukrspecsystems SharkDocument2 pagesLiflet Ukrspecsystems SharktwinksemeyPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Lakshamaner ShaktishelDocument19 pagesLakshamaner ShaktishelkundusumnaPas encore d'évaluation
- Area Address Contact - 1 Contact - 2 Number - 1 Number - 2 Company NameDocument16 pagesArea Address Contact - 1 Contact - 2 Number - 1 Number - 2 Company NameJoshua M. GenoviaPas encore d'évaluation
- Crossing The River by Feeling The Stones Deng Xiaoping in The Making of Modern ChinaDocument9 pagesCrossing The River by Feeling The Stones Deng Xiaoping in The Making of Modern ChinaVICTOR MBEBEPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- वृत्ति मार्गनिर्देशन तथा रोजगार मेला आयोजन कार्यविधि-२०७९Document19 pagesवृत्ति मार्गनिर्देशन तथा रोजगार मेला आयोजन कार्यविधि-२०७९Ganga Bdr BishwakarmaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Interceptor Ace Final 9.5 ProofDocument13 pagesInterceptor Ace Final 9.5 ProofPeter McGlonePas encore d'évaluation
- 1896 Philippine RevolutionDocument44 pages1896 Philippine Revolutionaj bPas encore d'évaluation
- Royal Moroccan Navy - BarcosDocument2 pagesRoyal Moroccan Navy - BarcosMario RubioPas encore d'évaluation
- Armed ForcesDocument8 pagesArmed ForcesVIJAYALAKSHMIPas encore d'évaluation
- The Spire Issue 0Document27 pagesThe Spire Issue 0BobleeSwagger1250% (2)
- Archive Scans - FSS Designs 4 - Mamoru Nagano Art Work and Design Work - F.S.S. Characters XIIIDocument154 pagesArchive Scans - FSS Designs 4 - Mamoru Nagano Art Work and Design Work - F.S.S. Characters XIIIaimond612002Pas encore d'évaluation
- Mgp3401 - Babylon 5 Wargame - A Call To Arms - Fleet Lists, 2nd EditionDocument161 pagesMgp3401 - Babylon 5 Wargame - A Call To Arms - Fleet Lists, 2nd Editionsunhawk8883% (12)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Finest Hour PDFDocument278 pagesThe Finest Hour PDFbob100% (1)
- The 29 February Us-Iea Agreement and Implications For Ngos: Table of ContentsDocument18 pagesThe 29 February Us-Iea Agreement and Implications For Ngos: Table of ContentsM. Yaqub AhmadiPas encore d'évaluation
- Attendance 1 FDocument8 pagesAttendance 1 FJenelyn BorbonPas encore d'évaluation
- OceanofPDF - Com The Great Illusion - Norman AngellDocument313 pagesOceanofPDF - Com The Great Illusion - Norman Angellmuhammad.melbPas encore d'évaluation
- Babur-Class CorvetteDocument6 pagesBabur-Class CorvetteejgarciacabralPas encore d'évaluation
- Askari Bank Limited: S.No Date RCVD Colt Sr. NTN Exporter - Name City - Name Cheque Amount Iban No. Bank NameDocument6 pagesAskari Bank Limited: S.No Date RCVD Colt Sr. NTN Exporter - Name City - Name Cheque Amount Iban No. Bank NameUsman FarooqPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)