Vous aimerez peut-être aussi
- Common List of Cardiac DrugsDocument3 pagesCommon List of Cardiac DrugsTracy100% (2)
- Acid Base DisturbancesDocument34 pagesAcid Base DisturbancesTracy100% (1)
- Intravenous Fluid SelectionDocument12 pagesIntravenous Fluid SelectionTracy100% (4)
- Common Cardiac Related MedicationsDocument18 pagesCommon Cardiac Related MedicationsTracy100% (2)
- Bipolar Mood ChartDocument2 pagesBipolar Mood ChartTracyPas encore d'évaluation
- ABG Interpretation: Julie Perkins RRT-NPS LPCH Respiratory CareDocument14 pagesABG Interpretation: Julie Perkins RRT-NPS LPCH Respiratory CareTracy100% (4)
- Abg InterpretationDocument14 pagesAbg Interpretationmara5140100% (7)
- Cardiac Meds To MemorizeDocument4 pagesCardiac Meds To MemorizekellyaePas encore d'évaluation
- Patient Procedures SurgeriesDocument4 pagesPatient Procedures SurgeriesTracyPas encore d'évaluation
- Patient Implantable Medical DevicesDocument1 pagePatient Implantable Medical DevicesTracy100% (1)
- Mania-Nursing Care PlanDocument2 pagesMania-Nursing Care PlanTracy74% (34)
- Cardiovascular DrugsDocument22 pagesCardiovascular DrugsTracy100% (1)
- Documenting A Transfusion Reaction: Chart SmartDocument2 pagesDocumenting A Transfusion Reaction: Chart SmartTracyPas encore d'évaluation
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Alcohol Withdrawal Assessment SheetsDocument2 pagesAlcohol Withdrawal Assessment SheetsTracy100% (1)
- Types of PainDocument1 pageTypes of PainTracy100% (3)
- Late Onset PTSTDocument7 pagesLate Onset PTSTTracy100% (1)
- Appendix B: Clinical Institute Withdrawal Assessment For Alcohol (CIWA-A)Document2 pagesAppendix B: Clinical Institute Withdrawal Assessment For Alcohol (CIWA-A)Tracy100% (1)
- Nursing Care Plan GuideDocument1 pageNursing Care Plan GuideTracy100% (1)
- WhenTPN Is IndicatedDocument3 pagesWhenTPN Is IndicatedTracyPas encore d'évaluation
- Notes To Slideshow: How Does The Chronic Care Model Work?Document18 pagesNotes To Slideshow: How Does The Chronic Care Model Work?TracyPas encore d'évaluation
- Drug Calculation TutorialDocument13 pagesDrug Calculation TutorialTracyPas encore d'évaluation
- Soap NoteDocument2 pagesSoap Notetopopirate100% (4)
- Useful AbbreviationsDocument2 pagesUseful AbbreviationsTracyPas encore d'évaluation
- PAS Quick GuideDocument1 pagePAS Quick GuideTracyPas encore d'évaluation
- Cleft Lip and PalateDocument2 pagesCleft Lip and PalateTracy100% (1)
- Psychiatry OverviewDocument2 pagesPsychiatry OverviewTracyPas encore d'évaluation
- Cerebral PalsyDocument2 pagesCerebral PalsyTracy100% (1)
- Spina BifidaDocument2 pagesSpina BifidaTracy100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Mobil Oil v. DiocaresDocument2 pagesMobil Oil v. DiocaresAntonio Rebosa100% (2)
- Surgical Orthodontics Library DissertationDocument5 pagesSurgical Orthodontics Library DissertationNAVEEN ROY100% (2)
- How To Download Gateways To Democracy An Introduction To American Government Book Only 3Rd Edition Ebook PDF Ebook PDF Docx Kindle Full ChapterDocument36 pagesHow To Download Gateways To Democracy An Introduction To American Government Book Only 3Rd Edition Ebook PDF Ebook PDF Docx Kindle Full Chapterandrew.taylor131100% (22)
- Court Reviews Liability of Staffing Agency for Damages Caused by Employee StrikeDocument5 pagesCourt Reviews Liability of Staffing Agency for Damages Caused by Employee StrikeDenzhu MarcuPas encore d'évaluation
- IB Diploma Maths / Math / Mathematics IB DP HL, SL Portfolio TaskDocument1 pageIB Diploma Maths / Math / Mathematics IB DP HL, SL Portfolio TaskDerek Chan100% (1)
- Food and ReligionDocument8 pagesFood and ReligionAniket ChatterjeePas encore d'évaluation
- Accounting What The Numbers Mean 11th Edition Marshall Solutions Manual 1Document36 pagesAccounting What The Numbers Mean 11th Edition Marshall Solutions Manual 1amandawilkinsijckmdtxez100% (23)
- Problem Areas in The Inpatient DepartmentDocument2 pagesProblem Areas in The Inpatient DepartmentVineet AgarwalPas encore d'évaluation
- ScriptsDocument6 pagesScriptsDx CatPas encore d'évaluation
- Dhikr or Zikr or Remembrance of AllahDocument27 pagesDhikr or Zikr or Remembrance of AllahMd. Naim KhanPas encore d'évaluation
- SEIPIDocument20 pagesSEIPIdexterbautistadecember161985Pas encore d'évaluation
- v6c. Story of CarbonDocument12 pagesv6c. Story of CarbonJahangir AliPas encore d'évaluation
- Total Product Marketing Procedures: A Case Study On "BSRM Xtreme 500W"Document75 pagesTotal Product Marketing Procedures: A Case Study On "BSRM Xtreme 500W"Yasir Alam100% (1)
- How To Use Google FormsDocument126 pagesHow To Use Google FormsBenedict Bagube100% (1)
- History of Downtown San Diego - TimelineDocument3 pagesHistory of Downtown San Diego - Timelineapi-671103457Pas encore d'évaluation
- PORT DEVELOPMENT in MALAYSIADocument25 pagesPORT DEVELOPMENT in MALAYSIAShhkyn MnPas encore d'évaluation
- Special Blood CollectionDocument99 pagesSpecial Blood CollectionVenomPas encore d'évaluation
- Eco Orphanage: Model of Sustainability: 15 536 Words (Not Including Bibliography)Document78 pagesEco Orphanage: Model of Sustainability: 15 536 Words (Not Including Bibliography)Princess ManiquizPas encore d'évaluation
- Investigation of Cyber CrimesDocument9 pagesInvestigation of Cyber CrimesHitesh BansalPas encore d'évaluation
- The Greco-Turkish War of 1920-1922: Greece Seeks Territory in Asia MinorDocument14 pagesThe Greco-Turkish War of 1920-1922: Greece Seeks Territory in Asia MinorFauzan Rasip100% (1)
- Mitanoor Sultana: Career ObjectiveDocument2 pagesMitanoor Sultana: Career ObjectiveDebasish DasPas encore d'évaluation
- Consolidation of AccountsDocument14 pagesConsolidation of Accountsram_alaways0% (1)
- Organizational CultureDocument76 pagesOrganizational Culturenaty fishPas encore d'évaluation
- Midland County Board of Commissioners Dec. 19, 2023Document26 pagesMidland County Board of Commissioners Dec. 19, 2023Isabelle PasciollaPas encore d'évaluation
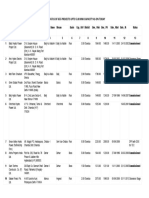
- List/Status of 655 Projects Upto 5.00 MW Capacity As On TodayDocument45 pagesList/Status of 655 Projects Upto 5.00 MW Capacity As On Todayganvaqqqzz21Pas encore d'évaluation
- 3 QDocument2 pages3 QJerahmeel CuevasPas encore d'évaluation
- Week 5 WHLP Nov. 2 6 2020 DISSDocument5 pagesWeek 5 WHLP Nov. 2 6 2020 DISSDaniel BandibasPas encore d'évaluation
- 4TH Quarter English 10 Assessment TestDocument6 pages4TH Quarter English 10 Assessment TestafbnjkcdPas encore d'évaluation
- A Brief History of The White Nationalist MovementDocument73 pagesA Brief History of The White Nationalist MovementHugenPas encore d'évaluation