Vous aimerez peut-être aussi
- Communication Disorders: Prevalence and Comorbid Intellectual Disability, Autism, and Emotional/Behavioral DisordersDocument9 pagesCommunication Disorders: Prevalence and Comorbid Intellectual Disability, Autism, and Emotional/Behavioral Disorderscoolblue89Pas encore d'évaluation
- Severe Impairments of Social Interaction PDFDocument19 pagesSevere Impairments of Social Interaction PDFjhernandez8394100% (1)
- New Developments in Autism Spectrum DisorderDocument14 pagesNew Developments in Autism Spectrum DisorderLuis Antonio HernándezPas encore d'évaluation
- Xcamouflaging in Autism SR Manuscript PrePrint 30.03.21Document52 pagesXcamouflaging in Autism SR Manuscript PrePrint 30.03.21Alexander OrzocoPas encore d'évaluation
- Family Matters (2005) Author: Reed, T (© Gender Identity Research and Education Society, GIRES) Families and Transsexualism - A Better UnderstandingDocument18 pagesFamily Matters (2005) Author: Reed, T (© Gender Identity Research and Education Society, GIRES) Families and Transsexualism - A Better UnderstandingSpongebob57Pas encore d'évaluation
- Experiences of Autism in Adulthood: A Qualitative Study (39 charactersDocument6 pagesExperiences of Autism in Adulthood: A Qualitative Study (39 charactersMirza Abdurehman ManiPas encore d'évaluation
- 559 FullDocument17 pages559 FullBobita BobiPas encore d'évaluation
- Autism Spectrum Disorder and Epigenetic LinksDocument12 pagesAutism Spectrum Disorder and Epigenetic LinksAndreea MarilenaPas encore d'évaluation
- Gillberg 2007 Adult DISCO LongitudinalDocument9 pagesGillberg 2007 Adult DISCO LongitudinalSkymaker69Pas encore d'évaluation
- Prevalence of Autism in A United States Population: The Brick Township, New Jersey, InvestigationDocument9 pagesPrevalence of Autism in A United States Population: The Brick Township, New Jersey, InvestigationSuci Triana PutriPas encore d'évaluation
- Diagnosis and Classification Autism DSMDocument29 pagesDiagnosis and Classification Autism DSMMaximiliano NoriaPas encore d'évaluation
- Literature Review by Shahir Samad Social ImpairmentDocument3 pagesLiterature Review by Shahir Samad Social ImpairmentirfanzukriPas encore d'évaluation
- Neurobehavioural and cognitive function linked to childhood trauma in homeless adultsDocument13 pagesNeurobehavioural and cognitive function linked to childhood trauma in homeless adultsReal NolosePas encore d'évaluation
- Psychopharmacology in Autism: UKE SAIDocument15 pagesPsychopharmacology in Autism: UKE SAIPablo Antonio AntonioPas encore d'évaluation
- Aula 2 - Material - How Many Doctors Does It Take To Make An Autism Spectrum DiagnosisDocument13 pagesAula 2 - Material - How Many Doctors Does It Take To Make An Autism Spectrum DiagnosistalitaPas encore d'évaluation
- Autism in Adolescents and Adults MesibovDocument23 pagesAutism in Adolescents and Adults MesibovSmurfing is FunPas encore d'évaluation
- A Parent-Report Instrument For Identifying One-Year-Olds Risk TEADocument20 pagesA Parent-Report Instrument For Identifying One-Year-Olds Risk TEADani Tsu100% (1)
- Aspergers in AdulthoodDocument12 pagesAspergers in AdulthoodNick Judson100% (1)
- DiscoDocument19 pagesDiscovcuadrosvPas encore d'évaluation
- Connor 41Document7 pagesConnor 41cta.catalunya8652Pas encore d'évaluation
- Areas: A Population Study Autism and Autistic-Like Conditions in Swedish Rural and UrbanDocument8 pagesAreas: A Population Study Autism and Autistic-Like Conditions in Swedish Rural and UrbanArvindan SubramaniamPas encore d'évaluation
- Huang WheelerDocument14 pagesHuang WheelerhengkitanjungPas encore d'évaluation
- Psychiatric Diagnosis Varies Across CulturesDocument8 pagesPsychiatric Diagnosis Varies Across CulturesPrisha SurtiPas encore d'évaluation
- Practice Parameter For The Assessment andDocument21 pagesPractice Parameter For The Assessment andBianca curveloPas encore d'évaluation
- Experiences in a Tertiary Care Hospital on Autism Diagnosis and ManagementDocument4 pagesExperiences in a Tertiary Care Hospital on Autism Diagnosis and ManagementSuppiah AnarsalamPas encore d'évaluation
- Puberty Suppression Medicine or MalpracticeDocument35 pagesPuberty Suppression Medicine or Malpracticebashomatsuo100% (1)
- King's Research Portal: 10.1038/nrurol.2016.128Document28 pagesKing's Research Portal: 10.1038/nrurol.2016.128Rafael MartinsPas encore d'évaluation
- Berto Glio 2009Document14 pagesBerto Glio 2009Jose Alonso Aguilar ValeraPas encore d'évaluation
- Use of The ADOS and ADI-R in Children With PsychosisDocument25 pagesUse of The ADOS and ADI-R in Children With PsychosiscaristaPas encore d'évaluation
- 1.ReceptiveandExpressiveLanguage ASDDocument47 pages1.ReceptiveandExpressiveLanguage ASDMUHAMMAD HAIKALPas encore d'évaluation
- J Schres 2011 11 037Document6 pagesJ Schres 2011 11 037teresa aloPas encore d'évaluation
- Stone 1987Document16 pagesStone 1987Στέργιος ΚPas encore d'évaluation
- Prevalence of SleepwalkingDocument4 pagesPrevalence of SleepwalkingPD11Pas encore d'évaluation
- Ajp 154 2 185Document6 pagesAjp 154 2 185fanzefirlPas encore d'évaluation
- Autism. TL 2014Document15 pagesAutism. TL 2014jujucastellPas encore d'évaluation
- Lovaas 1987Document15 pagesLovaas 1987intermetaparadigmatico6205Pas encore d'évaluation
- 10 1002@eat 23236Document12 pages10 1002@eat 23236LucíaPas encore d'évaluation
- GeneticHeritability 2011 07 04Document8 pagesGeneticHeritability 2011 07 04Ni Mas Ayu GandasariPas encore d'évaluation
- CBCL Profiles of Children and Adolescents With Asperger Syndrome - A Review and Pilot StudyDocument12 pagesCBCL Profiles of Children and Adolescents With Asperger Syndrome - A Review and Pilot StudyWildan AnrianPas encore d'évaluation
- Behavioral Treatment and Normal Educational and Intellectual Functioning in /bung Autistic ChildrenDocument7 pagesBehavioral Treatment and Normal Educational and Intellectual Functioning in /bung Autistic ChildrenMariaPas encore d'évaluation
- Theoretical Aspects of Autism: Causes-A Review: ReviewarticleDocument12 pagesTheoretical Aspects of Autism: Causes-A Review: ReviewarticleVe RenaPas encore d'évaluation
- Autism Spectrum Disorder GuideDocument100 pagesAutism Spectrum Disorder Guideام اسامة السيايدةPas encore d'évaluation
- Articol AutismDocument5 pagesArticol AutismOanaFloreaPas encore d'évaluation
- Adults With Autism - Changes in Understanding Since DSM-111 2Document18 pagesAdults With Autism - Changes in Understanding Since DSM-111 2maria fernanda avendañoPas encore d'évaluation
- Diagnosing Autism Spectrum Disorders: A Lifespan PerspectiveD'EverandDiagnosing Autism Spectrum Disorders: A Lifespan PerspectivePas encore d'évaluation
- Autism Longitudinal StudyDocument10 pagesAutism Longitudinal Studychristschool1440Pas encore d'évaluation
- Describing The Profile of Diagnostic Features in ADocument12 pagesDescribing The Profile of Diagnostic Features in AvcuadrosvPas encore d'évaluation
- Autism AssignmentDocument16 pagesAutism AssignmentKevin Muyekho100% (1)
- HolandaDocument11 pagesHolandaAlvaro Bejarano MartinPas encore d'évaluation
- Hearing Assessment in Co-Existing Condition With Developmental DisordersDocument43 pagesHearing Assessment in Co-Existing Condition With Developmental DisordersMSc Audio BPas encore d'évaluation
- SEXUAL BEHAVIOR IN AUTISM SPECTRUM DISORDERSDocument26 pagesSEXUAL BEHAVIOR IN AUTISM SPECTRUM DISORDERSNicholasPas encore d'évaluation
- Recognition and Treatment of Asperger Syndrome in The CommunityDocument22 pagesRecognition and Treatment of Asperger Syndrome in The Communitybdalcin5512Pas encore d'évaluation
- Understanding Autism Through Family PerspectivesDocument16 pagesUnderstanding Autism Through Family PerspectivesMichael BarnesPas encore d'évaluation
- Advice for Parents of Young Autistic ChildrenDocument13 pagesAdvice for Parents of Young Autistic ChildrenzakiahfPas encore d'évaluation
- Why We Should Study The Broader Autism Phenotype in Typically Developing PopulationsDocument13 pagesWhy We Should Study The Broader Autism Phenotype in Typically Developing PopulationsAna Luiza Ferreira PsiPas encore d'évaluation
- Confusion Between Depression and Autism in A High Functioning ChildDocument14 pagesConfusion Between Depression and Autism in A High Functioning ChildClaudia MihaiPas encore d'évaluation
- Pervasive Developmental Disorders in Preschool Children: Original ContributionDocument7 pagesPervasive Developmental Disorders in Preschool Children: Original ContributionrachelrojPas encore d'évaluation
- Prevalence of Schizophrenia Among Patients Admitted Into Neuro-Psychiatric Hospital, Rumuigbo, Port Harcourt, Rivers State, NigeriaDocument9 pagesPrevalence of Schizophrenia Among Patients Admitted Into Neuro-Psychiatric Hospital, Rumuigbo, Port Harcourt, Rivers State, NigeriaSteven JonesPas encore d'évaluation
- CHAPTER 02, Literature ReviewDocument27 pagesCHAPTER 02, Literature ReviewAyesha ArshedPas encore d'évaluation
- Visual attention to social and non-social objects across the autism spectrumD'EverandVisual attention to social and non-social objects across the autism spectrumPas encore d'évaluation
- Universal Measuring Instruments: TNM 34XxDocument6 pagesUniversal Measuring Instruments: TNM 34XxAngel RuizPas encore d'évaluation
- Namaste IndiaDocument12 pagesNamaste IndiaUtkarsh Pandey50% (2)
- A tour of a mysterious mansion and its surroundingsDocument4 pagesA tour of a mysterious mansion and its surroundingsSesshomaruHimuraPas encore d'évaluation
- Transmission Line TowersDocument3 pagesTransmission Line TowersSoumik Dandapat100% (2)
- Cultural Web NHS StrategyDocument4 pagesCultural Web NHS StrategyÄßħīłăşħ ĹăĐĐüPas encore d'évaluation
- Security in Project FinanceDocument25 pagesSecurity in Project FinanceIshaya AmazaPas encore d'évaluation
- x2 Electric Bike ManualDocument16 pagesx2 Electric Bike ManualwroxtarPas encore d'évaluation
- Lrfdcons 3 I3Document29 pagesLrfdcons 3 I3RAIMUNDO SUHERDINPas encore d'évaluation
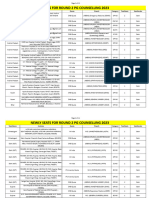
- Newly Seats For Round 2 PG Counselling 2023Document11 pagesNewly Seats For Round 2 PG Counselling 2023Manoj KumarPas encore d'évaluation
- UNILIA CURRICURUM VITAE - Mwayi ChirwaDocument5 pagesUNILIA CURRICURUM VITAE - Mwayi ChirwaBRIGHT TEMBOPas encore d'évaluation
- P180 Avanti-Pressurization SystemDocument4 pagesP180 Avanti-Pressurization SystemK M Mosheur RahmanPas encore d'évaluation
- Practical 1: Determination of Reducing Sugar Using The Dinitrosalicylic (DNS) Colourimetric MethodDocument8 pagesPractical 1: Determination of Reducing Sugar Using The Dinitrosalicylic (DNS) Colourimetric MethodNurSyazaHaniPas encore d'évaluation
- Genetics Case Study - MicrocephalyDocument4 pagesGenetics Case Study - MicrocephalyHeru WPas encore d'évaluation
- Review Materials: Prepared By: Junior Philippine Institute of Accountants UC-Banilad Chapter F.Y. 2019-2020Document19 pagesReview Materials: Prepared By: Junior Philippine Institute of Accountants UC-Banilad Chapter F.Y. 2019-2020AB CloydPas encore d'évaluation
- Dynapac CA500 Operation EssentialsDocument28 pagesDynapac CA500 Operation EssentialsalexandrePas encore d'évaluation
- 20 đề ôn thi học kỳ 2 môn tiếng anh 6Document59 pages20 đề ôn thi học kỳ 2 môn tiếng anh 6Tú BíPas encore d'évaluation
- Ingles - Currinculum Vitae AdoDocument7 pagesIngles - Currinculum Vitae Adomungueze domingosPas encore d'évaluation
- Handbook For Starting A New Community Garden - Community Action Coalition, WisconsinDocument22 pagesHandbook For Starting A New Community Garden - Community Action Coalition, Wisconsinfriends of the Native Plant Society of New Mexico0% (1)
- Creamery Juice HACCP PlanDocument27 pagesCreamery Juice HACCP PlanDavid ChanPas encore d'évaluation
- Problems-Convection 1Document2 pagesProblems-Convection 1Ira Octavia100% (1)
- DPI Report On WCPSS IDEA ComplianceDocument10 pagesDPI Report On WCPSS IDEA ComplianceKeung HuiPas encore d'évaluation
- Pumpable Shotcrete in LadleDocument9 pagesPumpable Shotcrete in LadlePartha Pratim Singha RoyPas encore d'évaluation
- Manual Tester 38XR-B PDFDocument4 pagesManual Tester 38XR-B PDFSantiago Fabián BuesoPas encore d'évaluation
- Traction ContraindicationsDocument2 pagesTraction ContraindicationslaymanzPas encore d'évaluation
- MoistScan 8pp Brochure LoResDocument8 pagesMoistScan 8pp Brochure LoResLuis PurisPas encore d'évaluation
- Carbon Black MoistureDocument14 pagesCarbon Black MoistureSanjay SurpuriyaPas encore d'évaluation
- Topic in Mental HealthDocument3 pagesTopic in Mental HealthSin ChiPas encore d'évaluation
- 02 Samss 012Document10 pages02 Samss 012bmkalePas encore d'évaluation
- Methyl T-Butyl Ether (Mtbe) Production: A Comparison of Montmorillonite-Derived Catalysts With Ion-Exchange ResinDocument7 pagesMethyl T-Butyl Ether (Mtbe) Production: A Comparison of Montmorillonite-Derived Catalysts With Ion-Exchange ResinTrà ĐáPas encore d'évaluation
- Fazal Din Stock ControlDocument30 pagesFazal Din Stock ControlPadietPas encore d'évaluation