Vous aimerez peut-être aussi
- 201 - The Saggy Baggy Elephant - See, Hear, ReadDocument28 pages201 - The Saggy Baggy Elephant - See, Hear, ReadAndrew RukinPas encore d'évaluation
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- Histopathology ETASDocument89 pagesHistopathology ETASDr.Tawheed75% (4)
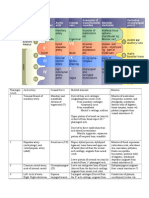
- Pharyngeal Arch Derivatives Chart!Document5 pagesPharyngeal Arch Derivatives Chart!Suphadetch Leung100% (1)
- GeneticsDocument13 pagesGeneticsNina SapphirePas encore d'évaluation
- Dictionary of Plant Biology En-SpDocument654 pagesDictionary of Plant Biology En-SpMelo2008100% (1)
- HEMODIALYSISDocument108 pagesHEMODIALYSISDan™100% (2)
- Hemodialysis: Carina Joane Villareal-Barroso, R.N.,M.NDocument108 pagesHemodialysis: Carina Joane Villareal-Barroso, R.N.,M.NJune BarsPas encore d'évaluation
- Acute Glomerulonephritis Case StudyDocument12 pagesAcute Glomerulonephritis Case StudyPrincess Tindugan100% (1)
- Under The Guidance Of: Dr. B.Shashidharan. Professor and Chief Unit-III By, Dr. Henley Punnen AndrewsDocument63 pagesUnder The Guidance Of: Dr. B.Shashidharan. Professor and Chief Unit-III By, Dr. Henley Punnen AndrewsHenley AndrewsPas encore d'évaluation
- Rembrandt BugattiDocument70 pagesRembrandt Bugattialdoremo1965100% (3)
- The Ontogenetic Basic of Human AnatomyDocument18 pagesThe Ontogenetic Basic of Human AnatomymeseniaPas encore d'évaluation
- Reproductive Biology and Phylogeny of SnakesDocument705 pagesReproductive Biology and Phylogeny of SnakesOscar David Ríos100% (2)
- ExcretionDocument17 pagesExcretionsmbdy tbhhhPas encore d'évaluation
- Urinalysis and Body FluidsDocument54 pagesUrinalysis and Body FluidsabdishakurPas encore d'évaluation
- Fluid and Electrolyte BalanceDocument3 pagesFluid and Electrolyte BalancejalajaraniPas encore d'évaluation
- A Share WATER & ELECTROLYTE BALANCEDocument14 pagesA Share WATER & ELECTROLYTE BALANCENaaz creates creativePas encore d'évaluation
- 25.9 Regulation of Fluid Volume and Composition - Anatomy and Physiology 2e - OpenStaxDocument4 pages25.9 Regulation of Fluid Volume and Composition - Anatomy and Physiology 2e - OpenStaxMarlene AngwaforPas encore d'évaluation
- 1.4 Virtual Patient - Elizabeth Harding: Describe The Structure of The NephronDocument7 pages1.4 Virtual Patient - Elizabeth Harding: Describe The Structure of The NephronAbdullah RajaPas encore d'évaluation
- Physio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionDocument5 pagesPhysio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionAnny AlvrzPas encore d'évaluation
- Biology Class NotesDocument11 pagesBiology Class NotessnnvcqzgnbPas encore d'évaluation
- Biology 7C 1Document4 pagesBiology 7C 1Abdullayev KamranPas encore d'évaluation
- 12.1 Waste Excretion and Equilibrium: Anatomy of The Urinary SystemDocument4 pages12.1 Waste Excretion and Equilibrium: Anatomy of The Urinary SystemVivian TangPas encore d'évaluation
- Excretion ExcretionDocument7 pagesExcretion ExcretionWaleed Bin KhalidPas encore d'évaluation
- Diagram of The KidneyDocument3 pagesDiagram of The KidneyElienai de LeonPas encore d'évaluation
- Test 4 Renal Gi Met DM AgingDocument9 pagesTest 4 Renal Gi Met DM AgingmeganPas encore d'évaluation
- THE URINARY SYSTEM Anatomy and PhysiologyDocument29 pagesTHE URINARY SYSTEM Anatomy and PhysiologyYatuwa LydiaPas encore d'évaluation
- Excretion (Continued)Document9 pagesExcretion (Continued)t0000123Pas encore d'évaluation
- Urinary Sys@completeDocument48 pagesUrinary Sys@completeGhina MengalPas encore d'évaluation
- The Renal SystemDocument10 pagesThe Renal SystemWahyu Purbo PangestiPas encore d'évaluation
- Basic of Fluid Therapy ImaDocument69 pagesBasic of Fluid Therapy Imal Made ArtawanPas encore d'évaluation
- PP24 Functioning of The KidneyDocument81 pagesPP24 Functioning of The KidneyLeloPas encore d'évaluation
- Chapter 16 ReviewDocument21 pagesChapter 16 Reviewjenn1722Pas encore d'évaluation
- The Human Excretory SystemDocument7 pagesThe Human Excretory Systemdonnah_veraPas encore d'évaluation
- KidneysDocument23 pagesKidneysshaliniPas encore d'évaluation
- Lecture 20 Notes 2018Document6 pagesLecture 20 Notes 2018Omed ZarifiPas encore d'évaluation
- FLG 332 Renal Physiology - 1 (2019)Document58 pagesFLG 332 Renal Physiology - 1 (2019)Huzaifa KhanPas encore d'évaluation
- 4 2 HomeworkDocument8 pages4 2 HomeworkShawntel IsordiaPas encore d'évaluation
- CairanDocument60 pagesCairanHanum HanattaPas encore d'évaluation
- Proximal Tubule Distal Tubule: Nutrients Nacl Hco H O K Nacl H O HcoDocument18 pagesProximal Tubule Distal Tubule: Nutrients Nacl Hco H O K Nacl H O HcogajenraoPas encore d'évaluation
- AP Biology Regulation Test ReviewDocument4 pagesAP Biology Regulation Test ReviewborntobewilderPas encore d'évaluation
- Chapter 19 Excretory Products and Their EliminationDocument27 pagesChapter 19 Excretory Products and Their Eliminationamit lakraPas encore d'évaluation
- Case AbstractDocument8 pagesCase AbstractRj DimaandalPas encore d'évaluation
- Fluid & Electrolyte Balance: Part 4: Regulation & MaintenanceDocument40 pagesFluid & Electrolyte Balance: Part 4: Regulation & MaintenanceMy MusicPas encore d'évaluation
- Endocrine Physiology: Dale Buchanan Hales, PHD Department of Physiology & BiophysicsDocument67 pagesEndocrine Physiology: Dale Buchanan Hales, PHD Department of Physiology & BiophysicsSourabh NandaPas encore d'évaluation
- PDF DocumentDocument86 pagesPDF DocumentRo-Anne LozadaPas encore d'évaluation
- Control of Extracellular Fluid Volume by The KidneyppDocument28 pagesControl of Extracellular Fluid Volume by The KidneyppLilian EdeniPas encore d'évaluation
- General Biology PPT Darryl Arcillas & Dency TuastumbanDocument14 pagesGeneral Biology PPT Darryl Arcillas & Dency TuastumbanApril Rose Caquilala GalauraPas encore d'évaluation
- AssignmentDocument6 pagesAssignmentleone shikukuPas encore d'évaluation
- JGLG TLA2 Refelective WritingDocument3 pagesJGLG TLA2 Refelective WritingJunnin Gay GarayPas encore d'évaluation
- The Renal SystemDocument53 pagesThe Renal SystemDarvey LongaraPas encore d'évaluation
- Renal Physiology 1Document9 pagesRenal Physiology 1Anny AlvrzPas encore d'évaluation
- Acute Glomerulonephritis Case StudyDocument12 pagesAcute Glomerulonephritis Case StudyPrincess Tindugan100% (1)
- Excretion and HomeostasisDocument11 pagesExcretion and HomeostasisstarcandypricessPas encore d'évaluation
- Chapter 25Document55 pagesChapter 25Chuy Cantu RdzPas encore d'évaluation
- I.Inroduction: Sign and SymptomsDocument7 pagesI.Inroduction: Sign and SymptomsMae Anne Cañas100% (1)
- 2d) Patofisiologi Sesak Napas by Dr. AminuddinDocument39 pages2d) Patofisiologi Sesak Napas by Dr. AminuddinMUHAMMAD BAGIR ALJUFRIPas encore d'évaluation
- Study Guide 2Document34 pagesStudy Guide 2api-260095216Pas encore d'évaluation
- Ii. Hydroelectrolytic Imbalance PDFDocument30 pagesIi. Hydroelectrolytic Imbalance PDFIvanes IgorPas encore d'évaluation
- Renal Physiology 5Document38 pagesRenal Physiology 5Hema KamatPas encore d'évaluation
- Physiology of Urine Formation: Submitted To - Mr. Pankaj Gupta Sir Department of ZoologyDocument15 pagesPhysiology of Urine Formation: Submitted To - Mr. Pankaj Gupta Sir Department of ZoologyRajeshwer duttPas encore d'évaluation
- The Urinary System: Pembentukan Urin Dan Peran Ginjal Dalam Keseimbangan Cairan TubuhDocument64 pagesThe Urinary System: Pembentukan Urin Dan Peran Ginjal Dalam Keseimbangan Cairan TubuhYunan Syahban MaskatPas encore d'évaluation
- SiadhDocument16 pagesSiadhGokul Rajan100% (1)
- 11.3 - The KidneyDocument7 pages11.3 - The KidneyraghadPas encore d'évaluation
- Clinical Disorder of Water 1Document7 pagesClinical Disorder of Water 1lovekhessyPas encore d'évaluation
- Renal Structure and Function: Dr. Catherine McdermottDocument38 pagesRenal Structure and Function: Dr. Catherine McdermottChrisPas encore d'évaluation
- Endocrine SystemDocument22 pagesEndocrine Systemmaxwell MutarePas encore d'évaluation
- Lower Limb Anatomy Quiz: Questions AnswersDocument3 pagesLower Limb Anatomy Quiz: Questions Answersapi-246259817Pas encore d'évaluation
- Upper Limb Anatomy Quiz: Questions AnswersDocument5 pagesUpper Limb Anatomy Quiz: Questions Answersapi-246259817Pas encore d'évaluation
- Year 1 Worksheet Wednesday 7Document1 pageYear 1 Worksheet Wednesday 7api-246259817Pas encore d'évaluation
- Head and Neck Quiz: Questions Answers My Answer Correct?Document6 pagesHead and Neck Quiz: Questions Answers My Answer Correct?api-246259817Pas encore d'évaluation
- Year 1 Worksheet Wednesday 8: CVRR Questions Are in RedDocument1 pageYear 1 Worksheet Wednesday 8: CVRR Questions Are in Redapi-246259817Pas encore d'évaluation
- Year 2 Worksheet Wednesday 6: 1. What Are The Three Parts of The Uterus?Document1 pageYear 2 Worksheet Wednesday 6: 1. What Are The Three Parts of The Uterus?api-246259817Pas encore d'évaluation
- Hi If Information On Potassium Levels Is Also Available Then You Should Use This in Your Calculation As Well. MarinaDocument1 pageHi If Information On Potassium Levels Is Also Available Then You Should Use This in Your Calculation As Well. Marinaapi-246259817Pas encore d'évaluation
- Year 1 Worksheet Wednesday 5: CVRR Questions Are in RedDocument2 pagesYear 1 Worksheet Wednesday 5: CVRR Questions Are in Redapi-246259817Pas encore d'évaluation
- Year 2 Worksheet Wednesday 5: CSIM Questions Are in BlueDocument1 pageYear 2 Worksheet Wednesday 5: CSIM Questions Are in Blueapi-246259817Pas encore d'évaluation
- UntitledDocument1 pageUntitledapi-246259817Pas encore d'évaluation
- Year 1 Worksheet Wednesday 2: CVRR Questions Are in RedDocument1 pageYear 1 Worksheet Wednesday 2: CVRR Questions Are in Redapi-246259817Pas encore d'évaluation
- Year 1 Worksheet Wednesday 6: CVRR Questions Are in RedDocument1 pageYear 1 Worksheet Wednesday 6: CVRR Questions Are in Redapi-246259817Pas encore d'évaluation
- Intro To Mic/ PPDDocument4 pagesIntro To Mic/ PPDapi-246259817Pas encore d'évaluation
- Year 1 Worksheet Wednesday 4: CVRR Questions Are in RedDocument1 pageYear 1 Worksheet Wednesday 4: CVRR Questions Are in Redapi-246259817Pas encore d'évaluation
- Shoulder Anatomy SummaryDocument4 pagesShoulder Anatomy Summaryapi-246259817Pas encore d'évaluation
- Year 2 Worksheet Wednesday 2: What Are The Different Categories of Differentiation of Malignant Neoplasms?Document1 pageYear 2 Worksheet Wednesday 2: What Are The Different Categories of Differentiation of Malignant Neoplasms?api-246259817Pas encore d'évaluation
- Year 1 Worksheet Wednesday 3: CVRR Questions Are in RedDocument1 pageYear 1 Worksheet Wednesday 3: CVRR Questions Are in Redapi-246259817Pas encore d'évaluation
- Introduction To FCDocument3 pagesIntroduction To FCapi-246259817Pas encore d'évaluation
- Year 2 Worksheet Wednesday 3: CSIM Questions Are in BlueDocument1 pageYear 2 Worksheet Wednesday 3: CSIM Questions Are in Blueapi-246259817Pas encore d'évaluation
- Year 1 Worksheet 1 AnswersDocument1 pageYear 1 Worksheet 1 Answersapi-246259817Pas encore d'évaluation
- Year 2 Worksheet Wednesday 1: CSIM Questions Are in BlueDocument1 pageYear 2 Worksheet Wednesday 1: CSIM Questions Are in Blueapi-246259817Pas encore d'évaluation
- Year 2 Worksheet 1 AnswersDocument1 pageYear 2 Worksheet 1 Answersapi-246259817Pas encore d'évaluation
- Year 1 Worksheet Wednesday 1: CVRR Questions Are in RedDocument1 pageYear 1 Worksheet Wednesday 1: CVRR Questions Are in Redapi-246259817Pas encore d'évaluation
- Reliability Theory of Aging and Longevity: Dr. Leonid A. Gavrilov, Ph.D. Dr. Natalia S. Gavrilova, PH.DDocument67 pagesReliability Theory of Aging and Longevity: Dr. Leonid A. Gavrilov, Ph.D. Dr. Natalia S. Gavrilova, PH.DUpendra KachruPas encore d'évaluation
- Altruism and Social TheoryDocument34 pagesAltruism and Social TheorySvetlanaPas encore d'évaluation
- Sri Chaitanya ZoologyDocument3 pagesSri Chaitanya ZoologypullaiPas encore d'évaluation
- MLTDocument20 pagesMLTSai SridharPas encore d'évaluation
- Wiki JellyfishDocument1 pageWiki Jellyfishwdm00Pas encore d'évaluation
- Cnidaria - Radiate Animals: HydrozoaDocument6 pagesCnidaria - Radiate Animals: Hydrozoafitness finessePas encore d'évaluation
- Animal ClassificationDocument18 pagesAnimal ClassificationPratham KhairnarPas encore d'évaluation
- EntomologyDocument50 pagesEntomologyapi-19960301100% (1)
- Biology Paper2 Form 4Document12 pagesBiology Paper2 Form 4hqbehPas encore d'évaluation
- Extinct Animals in India: Indian ChitaDocument4 pagesExtinct Animals in India: Indian ChitaHafizuddin SyedPas encore d'évaluation
- Hazel Rhs Horticulture Level 2 Essay 1Document24 pagesHazel Rhs Horticulture Level 2 Essay 1hazeldwyerPas encore d'évaluation
- Richard Dawkins in Furious Row With EO Wilson Over Theory of Evolution - Science - The GuardianDocument3 pagesRichard Dawkins in Furious Row With EO Wilson Over Theory of Evolution - Science - The GuardianrobiePas encore d'évaluation
- Examen - Unit 1 - Present SimpleDocument11 pagesExamen - Unit 1 - Present SimpleMary SalazarPas encore d'évaluation
- Work Sheet Animal Systematic I - Activity 2 - 20202021-1Document3 pagesWork Sheet Animal Systematic I - Activity 2 - 20202021-1Anang Yanuar RamadhanPas encore d'évaluation
- Rodriguez-Ferreretal - 2017 Marine RecorsDocument4 pagesRodriguez-Ferreretal - 2017 Marine Recorsalyman_bPas encore d'évaluation
- Migration in BirdsDocument29 pagesMigration in BirdsGEETA MOHAN100% (1)
- Z14 - Characteristics - Phylum Porifera & CnidariaDocument2 pagesZ14 - Characteristics - Phylum Porifera & CnidariaMilvy Faith C. SyjongtianPas encore d'évaluation
- Palaeoniscoid Remains From The Lower Permian Pedra de Fogo Formation Parna Ba Basin Insights From General Morphology and HistologyDocument12 pagesPalaeoniscoid Remains From The Lower Permian Pedra de Fogo Formation Parna Ba Basin Insights From General Morphology and HistologyVictor FontesPas encore d'évaluation
- Bingo สัตว์ 24คำDocument24 pagesBingo สัตว์ 24คำsatanghisoPas encore d'évaluation
- Skeleton Male or FemaleDocument5 pagesSkeleton Male or FemaleNaru DesuPas encore d'évaluation
- Chapter 18Document10 pagesChapter 18Aeriel Venice VergaraPas encore d'évaluation
- Bio205 Lab Report PDFDocument8 pagesBio205 Lab Report PDFjonahbsPas encore d'évaluation