Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Study Guide PathoPhysiology UCLA N 230 ADocument27 pagesStudy Guide PathoPhysiology UCLA N 230 ATracy Pope100% (1)
- 7 Mutation SCDocument54 pages7 Mutation SCThivya SritharPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Medical Genetics 4th Edition Jorde Test BankDocument4 pagesMedical Genetics 4th Edition Jorde Test BankOdettesPas encore d'évaluation
- Baker's YeastDocument9 pagesBaker's YeastRoshan Iyer100% (1)
- Genetic Disorders PDFDocument38 pagesGenetic Disorders PDFEllen Mae PrincipePas encore d'évaluation
- Biochem Genetics USMLE Practice Questions (2 of 4)Document13 pagesBiochem Genetics USMLE Practice Questions (2 of 4)MedSchoolStuff100% (2)
- Chromosomal AberrationsDocument20 pagesChromosomal Aberrationsvincentsharon0% (1)
- Pathophysiology Test Bank Ch. 2-4Document26 pagesPathophysiology Test Bank Ch. 2-4Joyy100% (3)
- Work and Social Adjustment Scale (W&sas)Document1 pageWork and Social Adjustment Scale (W&sas)Najia ChoudhuryPas encore d'évaluation
- Formulation: A Multiperspective Model : TermDocument8 pagesFormulation: A Multiperspective Model : TermNajia ChoudhuryPas encore d'évaluation
- Yale-Brown Obsessive Compulsive Scale (Y-BOCS)Document1 pageYale-Brown Obsessive Compulsive Scale (Y-BOCS)Najia ChoudhuryPas encore d'évaluation
- Borderline Personality ScreenerDocument2 pagesBorderline Personality ScreenerHannah HayesPas encore d'évaluation
- Brain Stimulation in Psychiatry by Kellner PDFDocument1 pageBrain Stimulation in Psychiatry by Kellner PDFNajia ChoudhuryPas encore d'évaluation
- Cat Eye Syndrome Associated With Aganglionosis of The Small and Large IntestineDocument2 pagesCat Eye Syndrome Associated With Aganglionosis of The Small and Large IntestineNajia ChoudhuryPas encore d'évaluation
- Kellner Flyer R1 PDFDocument1 pageKellner Flyer R1 PDFNajia ChoudhuryPas encore d'évaluation
- Kellner Flyer R1 PDFDocument1 pageKellner Flyer R1 PDFNajia ChoudhuryPas encore d'évaluation
- A Hereditary Bisatellite-Dicentric Supernumerary Chromosome PDFDocument4 pagesA Hereditary Bisatellite-Dicentric Supernumerary Chromosome PDFNajia ChoudhuryPas encore d'évaluation
- Social Anxiety Disorder Interventions For Adults With Social Anxiety DisorderDocument17 pagesSocial Anxiety Disorder Interventions For Adults With Social Anxiety DisorderNajia ChoudhuryPas encore d'évaluation
- Cat Eye Syndrome Owing To Tetrasomy 22pter Leads To q11 PDFDocument4 pagesCat Eye Syndrome Owing To Tetrasomy 22pter Leads To q11 PDFNajia ChoudhuryPas encore d'évaluation
- Cat-Eye Syndrome With Isolated Idiopathic Hypogonadotropic HypogonadismDocument5 pagesCat-Eye Syndrome With Isolated Idiopathic Hypogonadotropic HypogonadismNajia ChoudhuryPas encore d'évaluation
- A 600 KB Triplication in The Cat Eye Syndrome Critical Region Causes Anorectal, Renal and Preauricular Anomalies in A Three-Generation Family PDFDocument4 pagesA 600 KB Triplication in The Cat Eye Syndrome Critical Region Causes Anorectal, Renal and Preauricular Anomalies in A Three-Generation Family PDFNajia ChoudhuryPas encore d'évaluation
- Perimenstrual Psychiatric Hospitalization Case Report and Literature ReviewDocument7 pagesPerimenstrual Psychiatric Hospitalization Case Report and Literature ReviewNajia ChoudhuryPas encore d'évaluation
- Trisomy 22 With 'Cat Eye' Anomaly PDFDocument3 pagesTrisomy 22 With 'Cat Eye' Anomaly PDFNajia ChoudhuryPas encore d'évaluation
- Recurrent Psychotic Episodes With A Near - Monthly CycleDocument4 pagesRecurrent Psychotic Episodes With A Near - Monthly CycleNajia ChoudhuryPas encore d'évaluation
- Quick Reference Guide October 2010Document2 pagesQuick Reference Guide October 2010Najia ChoudhuryPas encore d'évaluation
- The Aetiology of The Cat Eye Syndrome Reconsidered PDFDocument12 pagesThe Aetiology of The Cat Eye Syndrome Reconsidered PDFNajia ChoudhuryPas encore d'évaluation
- Kellner Flyer R1Document1 pageKellner Flyer R1Najia ChoudhuryPas encore d'évaluation
- Exacerbation of Psychosis During Perimenstrual Phase of Menstrual Cycle Systematic Review and Meta-AnalysisDocument13 pagesExacerbation of Psychosis During Perimenstrual Phase of Menstrual Cycle Systematic Review and Meta-AnalysisNajia ChoudhuryPas encore d'évaluation
- Menstrual PsychosisDocument3 pagesMenstrual PsychosisNajia ChoudhuryPas encore d'évaluation
- Quick Reference Guide October 2010Document2 pagesQuick Reference Guide October 2010Najia ChoudhuryPas encore d'évaluation
- Quick Reference Guide October 2010Document2 pagesQuick Reference Guide October 2010Najia ChoudhuryPas encore d'évaluation
- Brief Psychosis in The Premenstrual Phase in An Adolescent GirlDocument3 pagesBrief Psychosis in The Premenstrual Phase in An Adolescent GirlNajia ChoudhuryPas encore d'évaluation
- Quick Reference Guide October 2010Document2 pagesQuick Reference Guide October 2010Najia ChoudhuryPas encore d'évaluation
- Quick Reference Guide October 2010Document2 pagesQuick Reference Guide October 2010Najia ChoudhuryPas encore d'évaluation
- Brief Psychosis in The Premenstrual Phase in An Adolescent GirlDocument3 pagesBrief Psychosis in The Premenstrual Phase in An Adolescent GirlNajia ChoudhuryPas encore d'évaluation
- Australian Medical Council CAT MCQ Application and Scheduling Process SummaryDocument2 pagesAustralian Medical Council CAT MCQ Application and Scheduling Process SummaryNajia ChoudhuryPas encore d'évaluation
- The Aetiology of The Cat Eye Syndrome Reconsidered PDFDocument12 pagesThe Aetiology of The Cat Eye Syndrome Reconsidered PDFNajia ChoudhuryPas encore d'évaluation
- Phenotypic Variability of The Cat Eye Syndrome. Case Report and Review of The LiteratureDocument10 pagesPhenotypic Variability of The Cat Eye Syndrome. Case Report and Review of The LiteratureNajia ChoudhuryPas encore d'évaluation
- Alteraciones Cromosomicas Molecular GeneticsDocument14 pagesAlteraciones Cromosomicas Molecular GeneticsChristian AguirrePas encore d'évaluation
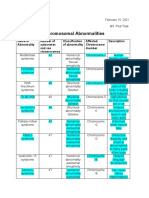
- EBIO-Table On Chromosomal Abnormalities-1Document2 pagesEBIO-Table On Chromosomal Abnormalities-1Alyanna Elisse VergaraPas encore d'évaluation
- W2023 BIO 1A03 DR Kajiura's Theme 5 M1 & M2 Applied LectureDocument38 pagesW2023 BIO 1A03 DR Kajiura's Theme 5 M1 & M2 Applied LectureSaajid AminPas encore d'évaluation
- Science: Quarter 3 - Module 5Document29 pagesScience: Quarter 3 - Module 5Amara VallePas encore d'évaluation
- Oral Pathology For The Dental Hygienist 7th Edition Ibsen Test BankDocument34 pagesOral Pathology For The Dental Hygienist 7th Edition Ibsen Test Banknopalsmuggler8wa100% (24)
- Product Sheet ChromoQuant PLUS E02Document2 pagesProduct Sheet ChromoQuant PLUS E02DEVESH BHOLEPas encore d'évaluation
- Adaptation To High Rates of Chromosomal Instability and Aneuploidy Through Multiple Pathways in Budding YeastDocument19 pagesAdaptation To High Rates of Chromosomal Instability and Aneuploidy Through Multiple Pathways in Budding YeastFernandoPas encore d'évaluation
- Biology Score: Chapter 7: MutationDocument15 pagesBiology Score: Chapter 7: MutationabbyPas encore d'évaluation
- Prenatal Testing in Genetic Mutation Carrrier ParentsDocument36 pagesPrenatal Testing in Genetic Mutation Carrrier ParentsJindal IVF ChandigarhPas encore d'évaluation
- Evaluation and management of recurrent pregnancy lossDocument30 pagesEvaluation and management of recurrent pregnancy lossSagar Shashikant BhavsarPas encore d'évaluation
- Bot Practical 10 Variation in Chromosome NumberDocument4 pagesBot Practical 10 Variation in Chromosome NumberAbdulrehmanPas encore d'évaluation
- TRN270532 Rubina-Pal 2694 275722 Panorama Report V1 PDFDocument3 pagesTRN270532 Rubina-Pal 2694 275722 Panorama Report V1 PDFSukhwinder KaurPas encore d'évaluation
- Genetic Disorders: Chromosomal Abnormalities and Down SyndromeDocument27 pagesGenetic Disorders: Chromosomal Abnormalities and Down SyndromeMerwan KemalPas encore d'évaluation
- MS Theses Abstracts PDFDocument48 pagesMS Theses Abstracts PDFMaureen GalapatePas encore d'évaluation
- Congenital Cytogenetic Abnormalities - UpToDateDocument34 pagesCongenital Cytogenetic Abnormalities - UpToDateIzamar RomeroPas encore d'évaluation
- General Embryology - 2Document71 pagesGeneral Embryology - 2danial zaffarPas encore d'évaluation
- Genetic MutationDocument27 pagesGenetic MutationKathleen JOy BiasUraPas encore d'évaluation
- Ch5 GeneticsDocument63 pagesCh5 GeneticsSrikanth Reddy VangaliPas encore d'évaluation
- Topic 6 - Imperfect Cause DefectDocument2 pagesTopic 6 - Imperfect Cause DefectSyaza Izzah Athirah Bt SpaieePas encore d'évaluation
- B.SC Botany Sem 5 6Document38 pagesB.SC Botany Sem 5 6Anonymous hN7XhLZuaIPas encore d'évaluation
- Module 8 - BS BiologyDocument10 pagesModule 8 - BS BiologyLeah MacadPas encore d'évaluation
- Genetics Canadian 2nd Edition Hartwell Test Bank 1Document24 pagesGenetics Canadian 2nd Edition Hartwell Test Bank 1robert100% (39)