Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- PROFESSIONAL Org-My SeminarDocument31 pagesPROFESSIONAL Org-My SeminarmariaPas encore d'évaluation
- Workplace Scars: Doctors' Mental HealthDocument6 pagesWorkplace Scars: Doctors' Mental HealthR. H.Pas encore d'évaluation
- Self-Harm and Suicide in Adults-2020Document83 pagesSelf-Harm and Suicide in Adults-2020geralddsackPas encore d'évaluation
- StarHealthAssureInsurancePolicy PolicyDocument20 pagesStarHealthAssureInsurancePolicy PolicyAnirudh SagaPas encore d'évaluation
- EdasdafsafDocument73 pagesEdasdafsafadi0077Pas encore d'évaluation
- Louisiana Inmate Search Department of Corrections LookupDocument7 pagesLouisiana Inmate Search Department of Corrections LookupinmatesearchinfoPas encore d'évaluation
- 27122021095025Document21 pages27122021095025jp2udhayaPas encore d'évaluation
- Local Conveyance Reimbursement FormDocument2 pagesLocal Conveyance Reimbursement FormHarDik PatelPas encore d'évaluation
- Analisis Penyebab Insiden Pasien Jatuh Di Rawat Inap Rs. Y Di Kota PadangDocument9 pagesAnalisis Penyebab Insiden Pasien Jatuh Di Rawat Inap Rs. Y Di Kota Padangjangmed rsghPas encore d'évaluation
- Tugas Bahasa Inggris Interview Irma & Tri 2C KepDocument2 pagesTugas Bahasa Inggris Interview Irma & Tri 2C KepTri mulyaniPas encore d'évaluation
- Q4 Health 10 Module 3Document20 pagesQ4 Health 10 Module 3anthonneacPas encore d'évaluation
- Approved Adv May 2023 - 5Document31 pagesApproved Adv May 2023 - 5edmund ndegwaPas encore d'évaluation
- Community-Led Health Equity Impact Assessment - Save Burdett CoalitionDocument32 pagesCommunity-Led Health Equity Impact Assessment - Save Burdett CoalitionRachel SilbersteinPas encore d'évaluation
- Mail Clerk Test V2 NewDocument4 pagesMail Clerk Test V2 NewDustin Neil SlomainyPas encore d'évaluation
- Selected Applicants To Attend Interview at Public Service Recruitment 18-23 NovemberDocument282 pagesSelected Applicants To Attend Interview at Public Service Recruitment 18-23 Novembermchaina Tv100% (1)
- 4Ps IssuesDocument2 pages4Ps IssuesMark Aldrin100% (1)
- The Health Care Delivery System CHN 1 Le PDFDocument49 pagesThe Health Care Delivery System CHN 1 Le PDFMariel TulaganPas encore d'évaluation
- Healthcare Delivery System of PakistanDocument4 pagesHealthcare Delivery System of PakistanRaheen AurangzebPas encore d'évaluation
- Community Based Health Care-1Document14 pagesCommunity Based Health Care-1Otema JamesPas encore d'évaluation
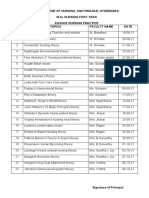
- JMJ College of Nursing, Snathnagar, Hyderabad M.SC Nursing First Year Advnce Nursing Practice S. No Topics Faculty Name DateDocument6 pagesJMJ College of Nursing, Snathnagar, Hyderabad M.SC Nursing First Year Advnce Nursing Practice S. No Topics Faculty Name DateRajani AshwinPas encore d'évaluation
- Quality of Care ArticleDocument6 pagesQuality of Care ArticleMostafa ElashryPas encore d'évaluation
- Zonal Employee Zed Fares Effective 01 Oct, 10Document3 pagesZonal Employee Zed Fares Effective 01 Oct, 10Muhammad NaveedPas encore d'évaluation
- Feature Paper in Antibiotics For 2019Document284 pagesFeature Paper in Antibiotics For 2019Felipe DonosoPas encore d'évaluation
- R MargabandhuDocument5 pagesR Margabandhuhhyd54vt59Pas encore d'évaluation
- PADILLO GROUP BSN 3E CHAPTER 1 3 Sir Jes 3Document61 pagesPADILLO GROUP BSN 3E CHAPTER 1 3 Sir Jes 3juliancheryll77Pas encore d'évaluation
- Healing Practices of Quack Doctors in The Health System in The PhilippinesDocument3 pagesHealing Practices of Quack Doctors in The Health System in The PhilippinesNadine EstorninosPas encore d'évaluation
- Benefit and Contribution ScheduleDocument75 pagesBenefit and Contribution SchedulejonaPas encore d'évaluation
- PMJAYPRIVATEHOSPITALSCONSOLIDATED 2-Converted12Document423 pagesPMJAYPRIVATEHOSPITALSCONSOLIDATED 2-Converted12Govarthanan DeepaPas encore d'évaluation
- Katherine Brown CVDocument6 pagesKatherine Brown CVapi-586798131Pas encore d'évaluation
- Nursing Research and Evidence Based Practice - EditedDocument3 pagesNursing Research and Evidence Based Practice - EditedHaya AwanPas encore d'évaluation