Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Meniscal TearDocument6 pagesMeniscal TearAdrian Diago TevesPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- OpiodsDocument10 pagesOpiodsAdrian Diago TevesPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Cerebrovascular Accident: DefinitionDocument8 pagesCerebrovascular Accident: DefinitionAdrian Diago TevesPas encore d'évaluation
- PNFDocument7 pagesPNFAdrian Diago TevesPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- 2017 OITE ReviewDocument105 pages2017 OITE ReviewJayPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Musculoskeletal Imaging Oxford HandbookDocument478 pagesMusculoskeletal Imaging Oxford HandbookJuned A Ansari100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Wrist and Hand ComplexDocument6 pagesWrist and Hand ComplexAlyssa Mae CamposanoPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Fundamental Movement PatternsDocument14 pagesFundamental Movement PatternsAnna Imaysay100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Clavicle, Sternum & Applied AnatomyDocument24 pagesClavicle, Sternum & Applied AnatomyBishal Chauhan100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Reactive Wall Push-Up: ExecutionDocument36 pagesReactive Wall Push-Up: Executioncoach_noePas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Weight Training Guide PDFDocument96 pagesWeight Training Guide PDFSam BlackPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Work Related Musculoskeletal Disorders in Physiotherapists Challenges and Coping Strategies WRMSDs in PhysiotherapistsDocument5 pagesWork Related Musculoskeletal Disorders in Physiotherapists Challenges and Coping Strategies WRMSDs in PhysiotherapistsInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Acl Reconstruction Rehab ProtocolDocument35 pagesAcl Reconstruction Rehab ProtocolCesar OliverosPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Week 2 & 4-8Document6 pagesWeek 2 & 4-8Lyrah SantuyoPas encore d'évaluation
- Dark Blue and Orange Fitness Gym Trifold BrochureDocument4 pagesDark Blue and Orange Fitness Gym Trifold BrochureKavya PandyaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Review Anatomi 4Document21 pagesReview Anatomi 4ajudPas encore d'évaluation
- Practice Questions 3 PDFDocument52 pagesPractice Questions 3 PDFKilopop Man100% (4)
- Chapter 6 Ergonomics and Safety Management PDFDocument57 pagesChapter 6 Ergonomics and Safety Management PDFdidievPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Scientific Programme PDFDocument20 pagesScientific Programme PDFChockalingam R MPas encore d'évaluation
- M T (DR Sadiq)Document62 pagesM T (DR Sadiq)DR-Muhammad ZahidPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Anatomical Terms of Movements or MotionDocument2 pagesAnatomical Terms of Movements or MotionThe BrodiePas encore d'évaluation
- Clinical Assessment of Musculoskeletal System-Handbook For MDocument36 pagesClinical Assessment of Musculoskeletal System-Handbook For MElqowiyyaPas encore d'évaluation
- Chap22-Shoulder ComplexDocument50 pagesChap22-Shoulder ComplextjPas encore d'évaluation
- Surface Anatomy: de La Salle-Lipa College of LawDocument79 pagesSurface Anatomy: de La Salle-Lipa College of LawFatzie MendozaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
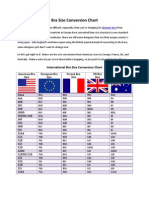
- Bra Size Conversion ChartDocument3 pagesBra Size Conversion ChartTop Drawer Lingerie100% (1)
- Tailore Story 1Document129 pagesTailore Story 1ghoongruPas encore d'évaluation
- Acetabular Fracture PostgraduateDocument47 pagesAcetabular Fracture Postgraduatekhalidelsir5100% (1)
- Femoral Neck FractureDocument32 pagesFemoral Neck FractureAndi Karwana Cipta100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Nine Jade Dragon ExerciseDocument4 pagesThe Nine Jade Dragon ExerciseSharma Men Ra60% (5)
- Shoulder JointDocument6 pagesShoulder JointDr santoshPas encore d'évaluation
- Current Views of Scapular Dyskinesis and Its Possible Clinical RelevanceDocument14 pagesCurrent Views of Scapular Dyskinesis and Its Possible Clinical RelevanceRoshani PPas encore d'évaluation
- Breast FeedingDocument6 pagesBreast FeedingPradhuymn MishraPas encore d'évaluation
- Level 3 - ExercisesDocument24 pagesLevel 3 - ExercisesTeamFrost ApplePas encore d'évaluation
- Applied Strongman Training Part 1Document48 pagesApplied Strongman Training Part 1shaft181100% (10)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)