Vous aimerez peut-être aussi
- Health Economics Note Chapter 12Document12 pagesHealth Economics Note Chapter 12Farian Tahrim VikiPas encore d'évaluation
- AHM 250 4 Provider CompensationDocument16 pagesAHM 250 4 Provider Compensationdeepakraj610Pas encore d'évaluation
- Health TermsDocument8 pagesHealth TermsHihiPas encore d'évaluation
- Chapter 5 - Provider Reimbursement MethodsDocument18 pagesChapter 5 - Provider Reimbursement MethodsAdityaPas encore d'évaluation
- Health Insurance 2Document32 pagesHealth Insurance 2roquiemayursaizPas encore d'évaluation
- On Health InsuranceDocument33 pagesOn Health InsuranceVenkat Reddy Arrabiri0% (1)
- Managed Health Care PlansDocument4 pagesManaged Health Care PlansShahidKumarPas encore d'évaluation
- Ahm 250 5 HmoDocument10 pagesAhm 250 5 Hmodeepakraj610Pas encore d'évaluation
- What Is An HMO Plan?Document8 pagesWhat Is An HMO Plan?fahhad lashariPas encore d'évaluation
- Textbook of Urgent Care Management: Chapter 22, Health Plan ContractingD'EverandTextbook of Urgent Care Management: Chapter 22, Health Plan ContractingPas encore d'évaluation
- Lva1 App6891Document63 pagesLva1 App6891Anil Kumar ARSPas encore d'évaluation
- Nsa Health Insurance BasicsDocument7 pagesNsa Health Insurance BasicsMaliPas encore d'évaluation
- Auc 5Document6 pagesAuc 5safPas encore d'évaluation
- Lva1 App6891Document63 pagesLva1 App6891Anil Kumar ARSPas encore d'évaluation
- What Is Managed CareDocument18 pagesWhat Is Managed CareYOGESHPas encore d'évaluation
- Health Economics - Lecture Ch12Document61 pagesHealth Economics - Lecture Ch12Katherine SauerPas encore d'évaluation
- Quiz NewDocument119 pagesQuiz NewMonyNaguPas encore d'évaluation
- Healthcare 101 An Introduction Day II - USTDocument59 pagesHealthcare 101 An Introduction Day II - USTAnonymous sthlPa7100% (1)
- PPN Statement Final January 2006Document2 pagesPPN Statement Final January 2006freaktonicPas encore d'évaluation
- HSM541 FinalDocument5 pagesHSM541 Finalteekel_1125Pas encore d'évaluation
- Topic 12 6 Course 2017-18Document12 pagesTopic 12 6 Course 2017-18Hikufe JesayaPas encore d'évaluation
- 3 Health Plan Benefits and NetworksDocument10 pages3 Health Plan Benefits and NetworksVinayaka KumarPas encore d'évaluation
- Basics of HealthCare DomainDocument4 pagesBasics of HealthCare DomainRajivPas encore d'évaluation
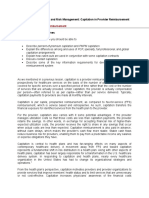
- Chapter 6 - Capitation in Provider ReimbursementDocument23 pagesChapter 6 - Capitation in Provider ReimbursementAdityaPas encore d'évaluation
- Textbook of Urgent Care Management: Chapter 40, Implementing Occupational MedicineD'EverandTextbook of Urgent Care Management: Chapter 40, Implementing Occupational MedicinePas encore d'évaluation
- Comparative Health Information Management 4th Edition Peden Solutions Manual 1Document13 pagesComparative Health Information Management 4th Edition Peden Solutions Manual 1daisy100% (32)
- Hospital Business ModelsDocument8 pagesHospital Business ModelsPOLOKO MHUSIWAPas encore d'évaluation
- Module 5 - Benifit Package DesignDocument13 pagesModule 5 - Benifit Package Design98b5jc5hgtPas encore d'évaluation
- Intro To Healthcare Study Guide - M3Document11 pagesIntro To Healthcare Study Guide - M3Juan David VargasPas encore d'évaluation
- Gail Carlson, MPH PH.D, State Health Education Specialist, University of Missouri ExtensionDocument9 pagesGail Carlson, MPH PH.D, State Health Education Specialist, University of Missouri ExtensionRahmat ShahPas encore d'évaluation
- Identifying and Resolving Disputes in New Accountable Care SettingsDocument10 pagesIdentifying and Resolving Disputes in New Accountable Care SettingsRothHealthLawPas encore d'évaluation
- Health Policy Brief: Accountable Care OrganizationsDocument6 pagesHealth Policy Brief: Accountable Care Organizationspalak32Pas encore d'évaluation
- Tanya Amon Assignment 2 HSA500Document5 pagesTanya Amon Assignment 2 HSA500Tanya Delaine AmonPas encore d'évaluation
- Assignment #1: Module 1: Assignment #1, Question #1 BUS 653Document5 pagesAssignment #1: Module 1: Assignment #1, Question #1 BUS 653Anna M SylvesterPas encore d'évaluation
- "Bundling" Payment For Episodes of Hospital CareDocument29 pages"Bundling" Payment For Episodes of Hospital CareCenter for American Progress100% (1)
- Ahm 250Document91 pagesAhm 250hemanthtikyani100% (1)
- AHM 250 3 Benefits & NetworksDocument13 pagesAHM 250 3 Benefits & Networksdeepakraj610Pas encore d'évaluation
- Private Third Party Prepayment PlansDocument25 pagesPrivate Third Party Prepayment PlansAbhishikth VarghesePas encore d'évaluation
- ACO Final ReportDocument24 pagesACO Final ReportSowmya ParthasarathyPas encore d'évaluation
- The Health Insurance WorkbookDocument12 pagesThe Health Insurance WorkbookLarry ThomasPas encore d'évaluation
- WP Insight HCR Impact On Rewards StrategiesDocument4 pagesWP Insight HCR Impact On Rewards StrategiesGeorge B. BuckPas encore d'évaluation
- NHISDocument36 pagesNHISCalista OdohPas encore d'évaluation
- Summary, Analysis & Review of Philip Moeller’s Get What’s Yours for MedicareD'EverandSummary, Analysis & Review of Philip Moeller’s Get What’s Yours for MedicarePas encore d'évaluation
- US HealthcareDocument3 pagesUS HealthcareRaghu TejaPas encore d'évaluation
- PUBH1382 Week 9 Content 2015 V3rDocument40 pagesPUBH1382 Week 9 Content 2015 V3rHammad -ullahPas encore d'évaluation
- Fan Understanding The Insurance ProcessDocument12 pagesFan Understanding The Insurance ProcessWill SackettPas encore d'évaluation
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersD'EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersPas encore d'évaluation
- President & CEO: Message From TheDocument7 pagesPresident & CEO: Message From Theneyj_8Pas encore d'évaluation
- Acknowledgement: Prof.B.P.Sharma Sir For Giving Me This Precious and Useful Opportunity To Improve MyDocument57 pagesAcknowledgement: Prof.B.P.Sharma Sir For Giving Me This Precious and Useful Opportunity To Improve MyDivyaroop HarshwalPas encore d'évaluation
- Fee For ServiceDocument5 pagesFee For Servicearun901Pas encore d'évaluation
- 2020 Health Benefit Summary PDFDocument36 pages2020 Health Benefit Summary PDFTitoPas encore d'évaluation
- Final Project For HINT 220Document16 pagesFinal Project For HINT 220Maxine WhitePas encore d'évaluation
- Payment in Healthcare OrganizationsDocument12 pagesPayment in Healthcare Organizationsevans kirimiPas encore d'évaluation
- 1.evolution of Heath PlansDocument9 pages1.evolution of Heath PlansUtpal Kumar PalPas encore d'évaluation
- AHM 250 Course MaterialDocument285 pagesAHM 250 Course MaterialAnitha Viji73% (15)
- 9 The Move To Consumer ChoiceDocument11 pages9 The Move To Consumer ChoiceVinayaka KumarPas encore d'évaluation
- The Best Laid Plans of Dogs and Vets: Transform Your Veterinary Practice Through Pet Health Care PlansD'EverandThe Best Laid Plans of Dogs and Vets: Transform Your Veterinary Practice Through Pet Health Care PlansPas encore d'évaluation
- Health Maintance Organization (HMO) Avena, Mma.: CDH 412 - DGCDocument8 pagesHealth Maintance Organization (HMO) Avena, Mma.: CDH 412 - DGCMary Margaret "MM" A. Avena0% (1)
- Parameter Weight Distribution For Selection at IIMsDocument3 pagesParameter Weight Distribution For Selection at IIMsSamir PrakashPas encore d'évaluation
- The Cultural Environments Facing BusinessDocument0 pageThe Cultural Environments Facing BusinessSamir PrakashPas encore d'évaluation
- EMI and The CT ScannerDocument5 pagesEMI and The CT ScannerSamir Prakash100% (1)
- Is There An Indian Way of ThinkingDocument19 pagesIs There An Indian Way of ThinkingSamir PrakashPas encore d'évaluation
- Companies With TaglinesDocument5 pagesCompanies With TaglinesSamir PrakashPas encore d'évaluation
- Team Bizdom Mica Samir Prakash Anjali Jain Abhishek Singh Mandloi Kunwarbir SinghDocument11 pagesTeam Bizdom Mica Samir Prakash Anjali Jain Abhishek Singh Mandloi Kunwarbir SinghSamir PrakashPas encore d'évaluation
- HCM 239Document199 pagesHCM 239Mohit VermaPas encore d'évaluation
- Viroguard Sanitizer SDS-WatermartDocument7 pagesViroguard Sanitizer SDS-WatermartIshara VithanaPas encore d'évaluation
- Topic 58 UKfrom1945Document10 pagesTopic 58 UKfrom1945Ana Giráldez RodríguezPas encore d'évaluation
- ETW-2013 Amma PDFDocument100 pagesETW-2013 Amma PDFRosalete LimaPas encore d'évaluation
- Development of A Taste-Masked Orodispersible FilmDocument12 pagesDevelopment of A Taste-Masked Orodispersible FilmKhoa DuyPas encore d'évaluation
- Antihypertensive Mcqs ExplainedDocument4 pagesAntihypertensive Mcqs ExplainedHawi BefekaduPas encore d'évaluation
- ABO Blood GroupDocument12 pagesABO Blood GroupGhost AnkanPas encore d'évaluation
- Comparative Analysis of National Pandemic Influenza Preparedness Plans - 2011Document64 pagesComparative Analysis of National Pandemic Influenza Preparedness Plans - 2011Mohamed WahbyPas encore d'évaluation
- Designated Structural Engineer Final 2016Document4 pagesDesignated Structural Engineer Final 2016Sri KalyanPas encore d'évaluation
- Presentation of Neurogenic Shock Within The Emergency Department - TaylorDocument6 pagesPresentation of Neurogenic Shock Within The Emergency Department - TaylorAnprtma kaunangPas encore d'évaluation
- African National Congress: Department of Information and PublicityDocument9 pagesAfrican National Congress: Department of Information and PublicityeNCA.com100% (2)
- 2005 Proverbs TOM SchizophreniaDocument7 pages2005 Proverbs TOM SchizophreniaKatsiaryna HurbikPas encore d'évaluation
- Clothier-Wright2018 Article DysfunctionalVoidingTheImportaDocument14 pagesClothier-Wright2018 Article DysfunctionalVoidingTheImportaMarcello PinheiroPas encore d'évaluation
- Estimation of Uric Acid Levels in SerumDocument6 pagesEstimation of Uric Acid Levels in Serumvicky_law_275% (4)
- Nso AblaparotomyDocument3 pagesNso AblaparotomyAleeya SarajanPas encore d'évaluation
- Form Lplpo Pustu Dan PoskesdesDocument3 pagesForm Lplpo Pustu Dan PoskesdesristiPas encore d'évaluation
- ProVari ManualDocument16 pagesProVari ManualPatrickPas encore d'évaluation
- Chinese Medicine Eng BrochureDocument12 pagesChinese Medicine Eng BrochuretanasedanielaPas encore d'évaluation
- Mangune v. Ermita (2016)Document3 pagesMangune v. Ermita (2016)Cristelle Elaine Collera100% (1)
- Health Beliefs and PracticesDocument7 pagesHealth Beliefs and Practicesapi-283426681Pas encore d'évaluation
- Nutritional Interventions PDFDocument17 pagesNutritional Interventions PDFLalit MittalPas encore d'évaluation
- Chapter One The History of BreathingDocument5 pagesChapter One The History of Breathingoiliver2011Pas encore d'évaluation
- An Atlas of Radiology of The Traumatized Dog and CatDocument566 pagesAn Atlas of Radiology of The Traumatized Dog and CatDenise Gomes de MeloPas encore d'évaluation
- SHARON SCHULTZ, ET AL. v. JANOS GUOTH, M.D. AND KHALED F. RABIE, M.D. (Parish of Rapides)Document18 pagesSHARON SCHULTZ, ET AL. v. JANOS GUOTH, M.D. AND KHALED F. RABIE, M.D. (Parish of Rapides)wstPas encore d'évaluation
- Professional Review Industry Route Guidance NotesDocument10 pagesProfessional Review Industry Route Guidance NotesAnonymous TlYmhkPas encore d'évaluation
- Review of The Health Benefits of Peas (Pisum Sativum L.) : Wendy J. Dahl, Lauren M. Foster and Robert T. TylerDocument8 pagesReview of The Health Benefits of Peas (Pisum Sativum L.) : Wendy J. Dahl, Lauren M. Foster and Robert T. TylerCrystal Joan D. MedranoPas encore d'évaluation
- Nupa BrochureDocument1 pageNupa BrochureLaboule KimozackPas encore d'évaluation
- Hazard Scale: 0 Minimal 1 Slight 2 Moderate 3 Serious 4 Severe Chronic HazardDocument4 pagesHazard Scale: 0 Minimal 1 Slight 2 Moderate 3 Serious 4 Severe Chronic HazardNazirAhmadBashiriPas encore d'évaluation
- Reactive Hyperplastic Lesions of The Oral CavityDocument8 pagesReactive Hyperplastic Lesions of The Oral CavityMarïsa CastellonPas encore d'évaluation
- Risk Assessment - GardenDocument2 pagesRisk Assessment - GardenOlivia BrookesPas encore d'évaluation