Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Anatomy and Physiology ReviewerDocument10 pagesAnatomy and Physiology Reviewermashup100% (14)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Candela CO2Re BRDocument8 pagesCandela CO2Re BRAlex ZPPas encore d'évaluation
- CASE STUDY 2011-CellulitisDocument34 pagesCASE STUDY 2011-Cellulitiscyrilcarinan75% (4)
- Encyclopedia of Dermatology 6 Volume Set PDFDocument1 880 pagesEncyclopedia of Dermatology 6 Volume Set PDFAlina BanicaPas encore d'évaluation
- المحاضرة الثانية تشريح اسنان م 1Document26 pagesالمحاضرة الثانية تشريح اسنان م 1mfhrluvxxxPas encore d'évaluation
- Nursing Management of The Burn-Injured PersonDocument44 pagesNursing Management of The Burn-Injured PersonKrina MarynaPas encore d'évaluation
- Anatomy & Physiology With Pathophysiology Lecture (Midterms)Document4 pagesAnatomy & Physiology With Pathophysiology Lecture (Midterms)Millen ArenasPas encore d'évaluation
- Asterias External FeaturesDocument23 pagesAsterias External Featuresyayeg rajaPas encore d'évaluation
- Phtsiology Hystology of The Skin. Primary & Secondary Morphological ElementsDocument21 pagesPhtsiology Hystology of The Skin. Primary & Secondary Morphological Elementsgrreddy8364320Pas encore d'évaluation
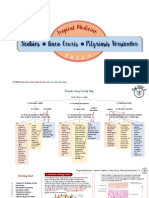
- Scabies Tinea Cruris Pityriasis Versicolor: Semangat!Document11 pagesScabies Tinea Cruris Pityriasis Versicolor: Semangat!Fitriah Nur SyamiatiPas encore d'évaluation
- Work Book Activity 9 Ana LabDocument7 pagesWork Book Activity 9 Ana LabJazmine YvonnePas encore d'évaluation
- Dermatological and Transdermal FormulationsDocument578 pagesDermatological and Transdermal FormulationsEdgardo Ed Ramirez50% (2)
- ANAPHY REVIEWER 4 Integumentary SystemDocument4 pagesANAPHY REVIEWER 4 Integumentary SystemJohn Niño CasuelaPas encore d'évaluation
- Porosity Analysis ImageJ PDFDocument8 pagesPorosity Analysis ImageJ PDFdibyodibakarPas encore d'évaluation
- Histo Lab Ex 13 17Document57 pagesHisto Lab Ex 13 17Allyzha AguilarPas encore d'évaluation
- Resurface and Peel Treatment TrainingDocument22 pagesResurface and Peel Treatment Trainingamymonuskin100% (6)
- Prescribing in DermatologyDocument142 pagesPrescribing in DermatologylaserPas encore d'évaluation
- VERUCCA VULGARIS PresentationDocument28 pagesVERUCCA VULGARIS PresentationBrilliantIbnuSina100% (2)
- FasciaeDocument54 pagesFasciaeSantiago Orihuela0% (1)
- Consensus Recommendations For The Use Of.2Document9 pagesConsensus Recommendations For The Use Of.2fregianiPas encore d'évaluation
- The Platelet Rich Plasma ProcedureDocument2 pagesThe Platelet Rich Plasma ProcedurekaisalanaafidaPas encore d'évaluation
- Biodamages and Protection of Leather and FurDocument11 pagesBiodamages and Protection of Leather and FurJUAN JOSE TUR MOYAPas encore d'évaluation
- Weber Sample Chapter 14Document34 pagesWeber Sample Chapter 14Sammy OhPas encore d'évaluation
- Image Gallery - Secondary Skin Lesions - Clinician's BriefDocument9 pagesImage Gallery - Secondary Skin Lesions - Clinician's BriefMabe AguirrePas encore d'évaluation
- SOAL UNAS Tahap 1 (TEORI) 22 Januari 2011 EdiDocument18 pagesSOAL UNAS Tahap 1 (TEORI) 22 Januari 2011 Ediandri perdanaPas encore d'évaluation
- Skin and Its AppendagesDocument7 pagesSkin and Its AppendagesSheena PasionPas encore d'évaluation
- Treat The Cause, Patient/Family and The Wound A Combination That Can Prove DifficultDocument33 pagesTreat The Cause, Patient/Family and The Wound A Combination That Can Prove Difficultcharity kalinowskyPas encore d'évaluation
- Physiology of INTEGUMENTARY SYSTEM FK PDFDocument84 pagesPhysiology of INTEGUMENTARY SYSTEM FK PDFdaris agharidPas encore d'évaluation
- Laser - Dr. Rômulo Meme (Livro Dr. Alcidarta Gadelha)Document18 pagesLaser - Dr. Rômulo Meme (Livro Dr. Alcidarta Gadelha)JoseJonatasPas encore d'évaluation
- Skin - Structure and Function Flashcards - QuizletDocument5 pagesSkin - Structure and Function Flashcards - QuizletDani AnyikaPas encore d'évaluation