Académique Documents
Professionnel Documents
Culture Documents
Educating For Teamwork Coordination in Simulated Cardiac Arrest Situations
Transféré par
Christina Barrett0 évaluation0% ont trouvé ce document utile (0 vote)
24 vues18 pagescardaic arrest
Titre original
Educating for Teamwork Coordination in Simulated Cardiac Arrest Situations
Copyright
© © All Rights Reserved
Formats disponibles
PDF, TXT ou lisez en ligne sur Scribd
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentcardaic arrest
Droits d'auteur :
© All Rights Reserved
Formats disponibles
Téléchargez comme PDF, TXT ou lisez en ligne sur Scribd
0 évaluation0% ont trouvé ce document utile (0 vote)
24 vues18 pagesEducating For Teamwork Coordination in Simulated Cardiac Arrest Situations
Transféré par
Christina Barrettcardaic arrest
Droits d'auteur :
© All Rights Reserved
Formats disponibles
Téléchargez comme PDF, TXT ou lisez en ligne sur Scribd
Vous êtes sur la page 1sur 18
ORI GI NAL RESEARCH
Educating for teamwork nursing students coordination
in simulated cardiac arrest situations
Sissel Eikeland Huseb, Hans Rystedt & Febe Friberg
Accepted for publication 15 January 2011
Correspondence to S.E. Huseb:
e-mail: sissel.i.husebo@uis.no
Sissel Eikeland Huseb MSc RN
PhD Student
University Lecturer
Department of Health Studies,
Faculty of Social Sciences,
University of Stavanger,
Norway
Hans Rystedt PhD RN
Senior Lecturer
Department of Education,
University of Gothenburg,
Sweden
Febe Friberg PhD RN
Associate Professor
Institute of Health and Care Sciences,
Sahlgrenska Academy at University of
Gothenburg, Sweden,
and
Department of Health Studies,
Faculty of Social Sciences,
University of Stavanger,
Norway
HUSEB S. E. , RYSTEDT H. & FRI BERG F. ( 2011) HUSEB S. E. , RYSTEDT H. & FRI BERG F. ( 2011) Educating for teamwork
nursing students coordination in simulated cardiac arrest situations. Journal of
Advanced Nursing 67(10), 22392255. doi: 10.1111/j.1365-2648.2011.05629.x
Abstract
Aim. The overarching aim was to explore and describe the communicative modes
students employ to coordinate the team in a simulation-based environment designed
for resuscitation team training.
Background. Verbal communication is often considered essential for effective
coordination in resuscitation teams and enhancing patient safety. Although simu-
lation is a promising method for improving coordination skills, previous studies
have overlooked the necessity of addressing the multifaceted interplay between
verbal and non-verbal forms of communication.
Method. Eighty-one nursing students participated in the study. The data were
collected in February and March, 2008. Video recordings from 28 simulated cardiac
arrest situations in a nursing programme were analysed. Firstly, all communicative
actions were coded and quantied according to content analysis. Secondly, inter-
action analysis was performed to capture the signicance of verbal and non-verbal
communication, respectively, in the moment-to-moment coordination of the team.
Findings. Three phases of coordination in the resuscitation team were identied:
Stating unconsciousness, Preparing for resuscitation, Initiating resuscitation. Coor-
dination of joint assessments and actions in these phases involved a broad range of
verbal and non-verbal communication modes that were necessary for achieving
mutual understandings of how to continue to the next step in the algorithm. This
was accomplished through a complex interplay of taking position, pointing and
through verbal statements and directives.
Conclusion. Simulation-based environments offer a promising solution in nursing
education for training the coordination necessary in resuscitation teams as they give
the opportunity to practice the complex interplay of verbal and non-verbal com-
munication modes that would otherwise not be possible.
Keywords: nursing education, nursing students, resuscitation, simulation-based
environment, team coordination, video recordings
2011 Blackwell Publishing Ltd 2239
J AN
JOURNAL OF ADVANCED NURSING
Introduction
Communication failure is responsible for up to 70% of all
patient error (Kohn et al. 2000), which is strongly related
to poor coordination among team members (Cooper &
Wakelam 1999, Xiao and the Lotas Group 2001, Grote et al.
2004). Nevertheless, the opportunities for team training in
healthcare education are seldom offered in the medical
and nursing education curricula (Kyrkjeb et al. 2006,
McConaughey 2008). Previous research has emphasized the
need for verbal communication to maintain effective coordi-
nation in resuscitation teams but very little research has been
done on how successful coordination takes place in simula-
tion-based environments (Manser et al. 2008). In the present
study, the research interest is extended to non-verbal com-
munication modes, such as gestures and body movements,
and the signicance of such modes in team members efforts
to coordinate their actions.
Mannequin-based simulations are increasingly used as
educational methods for training team skills (Anderson
2008). Such simulators include a computerized full-body
mannequin, which can be programmed to simulate the
physiological conditions of various medical disorders and
responses to the users interventions (Fritz et al. 2008).
Simulation thus allows for interactive and engaging activity
by recreating important aspects of a clinical event without
exposing patients to risk (Dieckmann 2009). Of central
concern in the present study is the potential of simulation
with a full-body mannequin to give opportunities for nursing
students to learn and practise team coordination skills.
Research on simulations indicates that training with manne-
quin-based simulators contributes to improved communica-
tion and teamwork on the part of nursing students, thus
leading to enhanced patient safety (Flanagan et al. 2004,
Medley & Horne 2005, Fritz et al. 2008). However, there is a
lack of knowledge concerning what aspects of the simulation-
based environment are critical for students development of
communication skills (Salas & Cannon-Bowers 2001).
Research on coordination within teams
In health care, coordination is an essential component of
successful teamwork (Manser et al. 2008, Salas et al. 2008).
The concept of coordination in the present study is under-
stood as the act of managing interdependencies between
activities performed by actors to achieve purposeful perfor-
mance (Hindmarsh & Pilnick 2002, 2007). However, few
studies have investigated team coordination in emergency
care and more research is needed to identify the conditions
necessary for the development of successful coordination in
simulation settings (Manser et al. 2008). Most of these
studies apply behavioural observation methods to the inves-
tigation of coordination within teams (Cooper & Wakelam
1999, Xiao and the Lotas Group 2001, Grote et al. 2004,
Manser et al. 2008). The results of these studies reveal that:
resuscitation teams need a coordination leader in order to
perform effectively (Cooper & Wakelam 1999), the require-
ment on coordination increases in line with task complexity
(Xiao and the Lotas Group 2001) and effective teams are
characterized by adapting their coordination strategies to the
requirements of the situation, i.e. employing more implicit
coordination in routine situations and more explicit coordi-
nation in critical situations (Grote et al. 2004).
One key nding in research on coordination is the
distinction between explicit and implicit coordination
(Manser et al. 2008). Explicit coordination refers to team
members use of clearly addressed messages to coordinate
actions (Serfaty et al. 1993), while implicit coordination is
based on a shared but tacit understanding of the task
requirements, which have usually been established in advance
(Wittenbaum et al. 1998). Some contradictions exist in
current research on coordination. On the one hand, a number
of studies suggest that implicit coordination is both prevalent
and effective in high workload situations where resources for
explicit coordination may be limited (Entin & Serfaty 1999,
Grote et al. 2004). On the other hand, research indicates that
lack of explicit coordination in critical situations leads to
coordination breakdowns (Xiao and the Lotas Group 2001).
It has also been claimed that explicit coordination is
associated with higher resuscitation team performance
(Cooper & Wakelam 1999, Tschan et al. 2006).
Explicit communication is one of the cornerstones of a
training programme called Crew Resource Management
(CRM) (for an overview, see Rall & Gaba 2005). CRM is
used in healthcare team training to promote safe and effective
communication among team members and is widely
acknowledged to enhance team performance (Rall &
Dieckmann 2005). Research demonstrates that CRM train-
ing produced positive reactions in trainees, although it has
been difcult to nd evidence for transfer to clinical settings
(Salas et al. 2006).
All research reported above investigated teamwork perfor-
mance by assessing verbal communication alone or verbal
and non-verbal communication as separate entities, while the
way in which speech and gestures are used simultaneously to
achieve coordination was not taken into account. In contrast,
the present study applies a research tradition rooted in
interaction analysis, which investigates the way in which
speech and bodily behaviour mutually constitute each other
in the organization and production of moment-to-moment
S.E. Huseb et al.
2240 2011 Blackwell Publishing Ltd
actions in real time (Goodwin 2000). These studies focus on
how team members establish a mutual understanding of the
situation at hand and how effective coordination of actions is
achieved on a collaborative level (Hindmarsh & Pilnick
2002, 2007). Hindmarsh and Pilnick (2002) demonstrated
how successful coordination between individuals was
achieved in anaesthesia teamwork. The ndings suggest that
the team members learn to read the implications of
embodied human behaviour for the specic demands of
teamwork. The results of Hindmarsh and Pilnicks (2007)
study show how the body constitutes an important resource
for effective real-time coordination in anaesthetic teamwork.
Both verbal and non-verbal responses are thus important for
displaying their understanding to each other about how to
continue with the task at hand (cf. Heath & Luff 1992).
Consequently, not only verbal communication has to be
addressed in order to understand the foundations of coordi-
nation of purposeful actions, but also non-verbal communi-
cation involving bodily aspects of human conduct. In line
with this research, the present study focuses on how students
interactively employ both verbal and non-verbal modes of
communication in coordinating joint actions in simulated
real-time tasks.
The study
Aim and research questions
The overarching aim of the study was to explore and describe
the communicative modes students employ to coordinate the
team in a simulation-based environment designed for resus-
citation team training. The following research questions
guided the analysis:
What is the signicance of verbal and non-verbal commu-
nication modes, respectively, and how do these interplay in
the coordination of resuscitation?
How do the students coordinate their activities to accom-
plish joint assessments and actions in the simulated resus-
citation team?
Methods
This study has an explorative and descriptive design (Polit
& Beck 2010). Observation through video recordings was
chosen due to the ability to capture complex interactions in
natural social settings (Heath et al. 2010). Video data
allow for different kinds of methodological approaches and
both a content analysis and an interaction analysis were
performed, which will be elaborated further in a section
that follows.
Participants
A total of 81 students (72 female and 9 male) in the last
semester of a 3-year nurse education programme, with an
average age of 27 years (range: 2253 years), participated in
the study. The students were divided into 14 groups, each of
which comprised in average six members. Both genders were
represented in four groups, whilst the rest consisted of female
students only. The average age of the groups varied from 23
to 33 years. The participant group was comparable with
other student groups in Norwegian nursing education
programme with respect to age and gender (Rykenes &
Larsen 2010). Five female faculty members aged between 34
and 60 (average age 49) with 2 years of experience in
simulation were involved as facilitators.
Ethical considerations
The study was approved by the Norwegian Social Science
Data Services (NSD) and the university. Consent forms were
signed by the nursing students and the faculty and conden-
tiality was guaranteed. All those who were asked agreed to
participate.
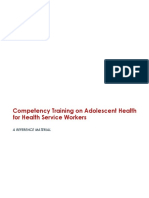
Setting
The study was performed in a simulation centre in Norway
using a patient simulator (SimMan) controlled by a monitor
located in an adjacent operator room. The mannequin that
was placed in a bed exhibited clinical signs such as palpable
pulses, breathing movements and sounds. A speaker located
in the mannequins head transmitted the voice of the
operator, thus giving the impression that the patient could
talk. The placement of the two video cameras (A and B) used
for the recordings can be seen in Figure 1. A microphone was
positioned in the ceiling.
The nursing students preparation prior to the simulation
session
Before starting the simulation session, the students attended
lectures about individual skills training in Basic life support
(BLS). According to European Resuscitation Guidelines from
2005, BLS refers to checking for response, opening the
airway to check for breathing and if absent, providing 30
chest compressions and two breaths (Handley et al. 2005)
(Figure 2).
Prior to the simulation session, each group was given a
brieng about the functioning of the mannequin. The
facilitator demonstrated how the medical equipment worked
JAN: ORIGINAL RESEARCH Educating for teamwork
2011 Blackwell Publishing Ltd 2241
and introduced the learning objective, i.e. teamwork training
for cardiac arrest situations. In this study the simulated
patient was a 71-year-old woman, who had suffered an upper
femur fracture and had been moved to the rehabilitation unit.
The patient had a history of angina pectoris.
At each simulation, the teams comprised three students.
They were instructed to act in a similar manner to that
used in the clinical eld during the 15-minute simulation.
The three remaining students in each group and the
facilitator were present in the room and observed the
simulation and in the next simulation scenario, the students
changed roles.
Data collection and analysis
The whole data material consisted of 28 hours of video
recordings of the simulated cardiac arrest events collected in
February and March 2008 by the rst author.
The video recordings were systematically reviewed with
focus on the students coordination of their activities. The
most demanding parts of employing the algorithm turned out
to be the rst three steps (Figure 2) which correspond to three
phases in the simulation scenarios: (1) stating unconscious-
ness, (2) preparing for resuscitation and (3) initiating resus-
citation. These parts, in all 28 groups, were transcribed (on
average 3 minutes, 48 seconds) to include each students
comments, gestures and actions and others responses to them.
A closer data analysis was performed in two steps. First,
content analysis was conducted to identify the form of
communicative actions occurring in all groups (Krippendorff
2004). All researchers (SEH, FF, HR) coded a selection of the
sequences together, and then the main author (SEH) coded
the whole data corpus. The entire coding was then discussed
among the authors until consensus was reached.
Further, all communicative actions were marked and coded
with respect to whether they involved (1) verbal, (2) non-
verbal and (3) simultaneous use of verbal and non-verbal
communication. In addition, these modes were divided with
respect to whether they concerned the accomplishment of
joint assessment or assembling joint actions. Secondly, the
number of all communication actions that occurred in the
data was counted. A full list of categories and numbers,
including examples, is given in Appendix 1.
In a second step, an interaction analysis was performed in
line with the recommendations of Heath et al. (2010) and
Jordan and Henderson (1995). Initially, collective analyses
were performed on seminars at the Linnaeus Centre for
Research on Learning, Interaction and mediated Communi-
cation (LinCS) in Sweden.
Recurrent patterns in the participants coordination of the
BLS algorithm were identied and specic attention was paid
to the interplay between different communication modes.
Three examples from one simulation session were selected for
a detailed analysis of the complexity of the interplay between
speech and gestures. These served as representative examples
of patterns of interaction in the sense that they illustrated the
28 simulations as a whole. By presenting an in-depth analysis
of one group it was possible to see how every new action was
based on previous activities of the group members (cf. Heath
& Luff 2000, Hindmarsh & Pilnick 2002).
D
e
s
k
B
Table
Door
Door
Chair Chair Chair
A
One-way-mirror
Operators chair
Figure 1 The simulation room.
Step 1. No movement or
response from the patient
Step 2. Open airway, check breathing
for 10 sec.
Step 3. If there is still no response and the
patient is not breathing normally, start 30
chest compressions
Step 4. Provide cycles of 30 compressions
and 2 rescue breathing
(Handley et al. 2005)
Figure 2 Basic life support (BLS).
S.E. Huseb et al.
2242 2011 Blackwell Publishing Ltd
Findings
The ndings are presented in the three phases identied,
corresponding to the three-rst steps in the BLS algorithm:
(1) Stating unconsciousness, (2) Preparing for resuscitation
and (3) Initiating resuscitation. Secondly, the result of
counting all the communication modes revealed certain
emerging patterns, which are described for all groups in each
phase. Thirdly, an in-depth analysis is presented of the same
phases, illustrating the complexity of the interplay between
different communication modes exhibited by the ndings.
Stating unconsciousness
In the event of a suspected cardiac arrest, the rst step in the
BLS algorithm is to check whether the patient is unconscious
(Figure 2). Identifying this point in time is critical, as it
signals when the next step in the algorithm should be carried
out. For the team to agree on this presupposes a mutual focus
achieved by a series of stepwise changes of position, enabling
close monitoring of the mannequins response to questions
and tactile stimulation. All of these actions place extensive
demands on the students to align themselves to each others
actions in a timely fashion.
Figure 3 shows the numbers of different communication
modes in the phase of stating unconsciousness. In this phase
we identied two subcategories: joint assessment and joint
action. Joint assessment subcategories imply that the patients
vital functions are monitored and identied while joint
actions imply actions to be taken to prepare for or to initiate
resuscitation. In all instances of verbal, non-verbal and
simultaneous use of both verbal and non-verbal communica-
tion, the subcategory joint assessment received the highest
number compared to that of joint action(153 vs. 34).
Examples of the simultaneous use of verbal and non-verbal
modes in the joint assessment subcategory were naming and
questioning the patient simultaneously with touching
and shaking the mannequin for a response. Verbally stating
the need to call 113 and doing it at the same time was an
example of using dual modes in assembling joint action
(Appendix 1).
How such coordination is enacted in detail is here shown
by foregrounding the activities of one of the groups. A typical
example is illustrated below (Figure 4), in which student 2
(S2) and student 3 (S3) stand on each side of the bed close to
the patient and student 1 (S1) is positioned in front of and
facing the desk occupied by the task of preparing an injection
(Figure 4i). The question Are you there- Brenda? by S3 is the
initial step in checking consciousness.
As the mannequin cannot simulate body movements or
skin colour changes, verbal response is the only means of
checking the level of consciousness (Figure 2, step 1). S3s
question Brenda, is everything okay with you?-hello (Fig-
ure 4ii) is thus a way of nding out whether there is any
response from the simulated patient. Shared attention is
seldom achieved immediately, but occurs in several steps.
This is illustrated in Figure 4i, in which S1 has assumed a
body orientation in front of and facing the desk, which means
that she was occupied by the task of preparing an injection.
S1 responds to S3s question by turning her head 90 degrees
towards the mannequin, while her torso and legs remain
oriented to the desk (ii). This body torque projects instability
in relation to the home position, which signals change so that
the head and torso will once again be brought into a
convergent alignment (Schegloff 1998). One second later S1
had rotated her body 160 and was now facing the bed,
glancing at the mannequin (iii). Although S1 was engaged in
another activity, she simultaneously monitored the actions of
her colleagues. In this case, the question Brenda, is every-
thing okay with you?-hello addressed by S3 to the manne-
quin triggered S1 to undertake the next step, i.e. to leave the
desk and move towards the bed. The lack of an answer to the
questions put to the mannequin and the stepwise changes in
position were thus essential in creating a shared focus on the
level of consciousness (Heath & Luff 1992). The absence of
an answer from the patient has an important meaning in this
particular setting in which checking consciousness is a part of
the familiar algorithm and unconsciousness is expected to
70
60
50
40
30
20
10
Verbal Nonverbal Verbal + Nonverbal
Joint assessment
Joint action
0
Figure 3 The total number of communi-
cation actions quantied within the
different communication modes in the
phase of stating unconsciousness.
JAN: ORIGINAL RESEARCH Educating for teamwork
2011 Blackwell Publishing Ltd 2243
occur. The problem here consists of identifying exactly when
this happens and when the next step should be initiated. In
turning away from less urgent tasks and towards the
mannequin, the students are able to indicate to each other
preparedness for the occurrence of this critical state.
A common pattern in the majority of groups was that the
students simultaneously combined verbal modes such as
naming and questioning with a demonstration of checking
with their senses to determine if the patient was unconscious.
The students seldom explicitly asked other students for help
or discussed what should be done in such situations. Overall,
this points to the fact that the interplay between verbal and
non-verbal communication is critical for agreeing on when
the simulated patient is unconscious.
Preparing for resuscitation
One part of applying the algorithm, although not addressed
in the model itself, is to prepare for and facilitate ventilation
and compressions by bending down the back rest, removing
the pillows and placing the patient in a prone position. Jointly
arranging for this position demands that the students are at
all times able to predict what subsequent actions they are
supposed to perform.
Figure 5 shows the numbers of communication modes in
the phase of preparing for resuscitation. Non-verbal com-
munication in the joint action subcategory received the
highest number compared to all other subcategories in
both verbal communication and simultaneous use of both
S3
The arrows illustrate the orientation of S1s head, torso and legs.
(3601) S1 is standing at the desk preparing an injection with her back to
the others. S2 is on the right side of the bed looking at the mannequin.S3 is
on the left with her hands on the mannequins shoulder, looking at the
mannequins face and asking Are you thereBrenda?. The patient does
not respond. S2 utters Brenda.
S1
S2
i
S3
(3604) Once again S3 tries to obtain a response by asking Brenda, is
everything okay with you? hello. S1 reacts to the lack of a response by
turning her head towards the mannequin without moving her torso and
legs.
S1
S2
(3605) S1 then takes one step forward towards the bed, glancing at the
mannequin. S2 says Hello Brenda.
ii
S3
S1
S2
iii
Figure 4 Stating unconsciousness.
S.E. Huseb et al.
2244 2011 Blackwell Publishing Ltd
communication modes (108 vs. 7). Examples of non-verbal
modes were when students gave each other space, as
demonstrated through their movements. Another example
of such actions is how they aligned themselves with each
others actions in simultaneously bending down the backrest
and then lifting up the mannequin to remove the pillows
(Appendix 1).
The interaction analysis of this phase reveals how the
students are regularly able to coordinate their assessments
and actions by positioning themselves very close to each other
around the bed. In this way, they were able to monitor each
others actions that did not require as much verbal commu-
nication as in the previous phase. This is illustrated in
Figure 6i, where S2 and S3 are standing on each side of the
bed and S1 has moved towards the bedside table to conduct
the next step, i.e. placing the patient in a prone position
(Figure 4i).
This initial spatial arrangement does not allow for eye
contact. Nor is there any verbal exchange between S1 and S3.
S1 does not request S3 to move to the right, nor does S3 ask if
she should move (ii). Instead S3 reads S1s body language
and uses it as a resource for attuning to her fellow student by
changing her own position (Hindmarsh & Pilnick 2002,
2007). Figure 6ii illustrates how the students regularly place
themselves very close to each other around the bed in ways
that facilitate the monitoring of each others actions. In other
words, they create a formation that gives the necessary
conditions for the effective exchange of glances, gestures and
words (Kendon 1990). The spatial arrangements establish
public, shared foci of visual and cognitive attention including
100
90
80
70
60
50
40
30
20
10
0
Verbal Nonverbal Verbal + Nonverbal
Joint assessment
Joint action
Figure 5 The total number of communi-
cation actions quantied within the
different communication modes in the
phase of preparing for resuscitation.
(3606) S1 walks towards the bedside table, moves it to the left and
places herself at the head of the bed. This position allows her to push
down the back of the bed to lay the patient flat.
(3607) When S3 notices that S1 has moved the bedside table and
placed her body between it and the bed, she shifts slightly to the right
to give S1 space in which to accomplish her task with the bed. S1
simultaneously issues the following instruction Lets see - take
down the back. S2 responds to S1s instruction by pushing the
handle and taking down the back of the bed from the right hand side.
They accomplish the task together and with parallel movements in
order to quickly position the patient horizontally.
S3
S3
S1
S1
S2
S2
i
ii
Figure 6 Preparing for resuscitation.
JAN: ORIGINAL RESEARCH Educating for teamwork
2011 Blackwell Publishing Ltd 2245
the mannequin with which they are working, and explains
the extensive use of non-verbal communication modes
(Figure 5). When giving the instruction Lets see take
down the back (ii) S1 uses the adverb down, indicating a
specic direction to the student behind the bed. Although the
recipient of the verbal directive is not explicitly mentioned by
name, S2s immediate response shows that she realized that it
was intended for her. S1s request Lets see take down the
back functions as a coordinating utterance that makes it
possible for the team to go ahead with the preparations for
cardiopulmonary resuscitation (CPR). Note that this action
occurs before the students had conrmed the absence of
breathing, which is the second step in the BLS algorithm
(Figure 2). The reversed order demonstrates that the students
anticipate a cardiac arrest and the actions that are supposed
to follow.
Initiating resuscitation
Steps 2 and 3 in the algorithm are to ensure that the airways
are open, to check breathing and to identify if absence of
response and breathing persist. This is a critical phase in
applying the algorithm since it serves as an indication of
cardiac arrest and signals the need to start CPR immediately
(Figure 2).
Figure 7 shows the number of the different communication
modes in the phase of initiating resuscitation. Joint action
received the highest number in all modes of communication,
indicating the need for starting CPR. Examples of assembling
joint actions included verbal directives to remove the head-
board or to ask for medical devices. Non-verbal communi-
cative modes mainly involved pointing at the oral airway or
the debrillator as a request to other team members to
retrieve or hand them over. Simultaneous use of verbal and
non-verbal communication included saying, for example,
you must connect the oxygen, at the same time as looking
and pointing at the oxygen device. Nevertheless, joint
assessment occurred frequently in this phase, and included,
for example, the interplay between conrming cardiac arrest
verbally and simultaneously removing the headboard or
medical devices (Appendix 1).
The last example shows in detail how the interplay of
verbal and non-verbal communication modes enabled them
to assess when the crucial signs of cardiac arrest were present
and how these, in turn, indicated the point of time at which
to take action (step 2 and 3 in the BLS algorithm) (Figure 8).
This point in time was preceded by actions such as inspecting,
listening and trying to sense chest heaves so that the others
could see them. It is noteworthy that the mannequins
inability to simulate breathing through the mouth means
that it is only possible to check for the absence of breathing
by a visual inspection and by means of the tactile senses (i).
Through the visible monitoring of the mannequins breath-
ing and simultaneous utterance No, she is not breathing, S3
gives the other participants with important information
about the patients ventilation status, which becomes avail-
able through temporal interplay between communicative
methods such as inspecting, sensing and listening. The
utterance is connected with a search for thorax movement
by leaning over the mannequin and simultaneously feeling for
breathing movements by laying the hand on the mannequins
chest. This indicates to the rest of the team that the proper
examinations have been conducted, while a remark about
ventilation status signals the need to continue. S1 responds by
removing the glasses from the mannequin, bending down,
glancing at its chest and reformulating S3s information
about the absence of breathing, now using a well-known
institutional term No breathing (ii). This, in turn, functions
as a signal for action. The statement indicates the start of
resuscitation and several other actions that are supposed to
follow in the BLS algorithm, i.e. preparation for ventilating
the patient and initiation of chest compression. The statement
No breathing changes the scenario from an everyday care to
a lifesaving activity, assuming that the timely actions set out
in the BLS algorithm are applied. In a similar vein as in the
preceding sequences, the mutual aligning to each others
actions and non-verbal communication modes forms the
basis for joint agreement on how to proceed. In addition, No
80
70
60
50
40
30
20
10
Verbal Nonverbal Verbal + Nonverbal
Joint assessment
Joint action
0
Figure 7 The total number of
communication actions quantied within
the different communication modes in the
phase of initiating resuscitation.
S.E. Huseb et al.
2246 2011 Blackwell Publishing Ltd
breathing serves as a denite signal for the team members to
start CPR.
Discussion
Limitations
Although the generality of the communication pattern found
in the present study are supported by the studies of other
healthcare teams, there might be some limitation to the
conclusions due to the fact that all students were recruited
from only one nursing programme in Norway. They may
differ from non-Norwegian students with respect to cultural
and educational background as well as gender and age. Even
though only the rst steps in the algorithm were analysed
(since these turned out to be most challenging for the
students) this may contribute in some part to understanding
coordination, alongside a study of all the steps.
Discussions of results
The ndings reveal three phases of coordination, stating
unconsciousness, preparing for resuscitation, initiating
resuscitation. Coordination of joint assessments and actions
in these phases involved a broad range of verbal and non-
verbal communication modes that were necessary for
achieving mutual understandings of how to continue to
the next step in the algorithm. This was accomplished
through a complex interplay of taking position, pointing,
and through verbal statements and directives. The results
reveal how the interplay between verbal and non-verbal
communication is vital in achieving coordination in teams.
Aligning to each others bodily movements and positions is
often enough to assemble joint actions. Joint assessments,
however, often require both verbal communications in
addition to non-verbal modes. The same applies, for
instance when prompt and timely actions are to be initiated,
such as at the start of CPR.
The result of counting all communication modes revealed
that verbal and non-verbal communications were essential
in joint assessment of when unconsciousness occurred and in
joint initiation of CPR. In a study on coordination in
anaesthesia it was showed that during assessment, planning
and decision-making the simultaneous use of verbal and non-
verbal communication were a prevalent coordination mech-
anism (Manser et al. 2008). The monitoring of other team
i
S3
S1
ii
S2
(3612) S3 places her right hand on the mannequins chest and bends
down to listen for breathing sounds, looking and feeling with her right
hand for thorax movements and saying No, she is not breathing.
(3619) S1 responds to S3s statement by removing the patients glasses,
bending down, glancing at the mannequins chest and verifying S3s
statement by saying No breathing. S3 responds by removing the duvet
and the kidney bowl from the mannequins torso.
S2
S1
S3
Figure 8 Initiating resuscitation.
JAN: ORIGINAL RESEARCH Educating for teamwork
2011 Blackwell Publishing Ltd 2247
members activities was also found to be salient, and
consistent with the ndings of the present study in the phase
of preparing for resuscitation. Our ndings are also consis-
tent with previous research on coordination, demonstrating
that non-verbal communication is effective in the coordina-
tion of high workload situations (Entin & Serfaty 1999,
Grote et al. 2004).
In all, our results are consistent with previous studies that
point to the necessity of training broader aspects of
coordination than mere verbal communication. Moreover,
a wide range of verbal and non-verbal modes of commu-
nication were necessary to agree on how to proceed and
how to perform joint and timely actions. This included
employing speech, gestures, eye contact, artefacts (the
mannequin) and the physical environment. The particular
set of resources available in the setting constituted the
conditions necessary for the students to align themselves to
each other (Goodwin 2000). The actions could not have
been performed without the students being able to perceive
each others bodily movements in combination with verbal
communication. Throughout the simulation session, the
different types of communication modes mutually comple-
mented each other, thus providing the basis for successfully
carrying out the steps of the BLS algorithm. The framing of
the situation as one in which the BLS algorithm should be
realized was another central condition for attributing
important meanings to speech, actions and artefacts. The
prompt response to the statement No breathing (Figure 8)
presupposes that its meaning is taken for granted by the
participants. In this way, the application of the algorithm
itself offers a context in which both directed speech and
indirect communication convey messages that are under-
stood in specic ways.
The relevance of simulation as an arena for training is
demonstrated by the fact that the team members communi-
cative actions for achieving coordination in the simulation
were very close to competent clinical teamwork. Hindmarsh
and Pilnick (2002, 2007) revealed how the body forms a
critical resource for successful coordination in anaesthesia
teamwork. Although many of the tasks carried out in the
practice of anaesthesia differ from those in the simulated
cardiac arrest situation, their characteristics are similar. The
students worked as a team, the task of which was to
collaboratively monitor and support the patients vital
functions. In contrast to Hindmarsh and Pilnicks (2002,
2007) ndings, the inexperienced students, who were not
trained in teamwork prior to the simulation, were unable to
rely on predened roles and a prearranged division of labour
to the same extent as professionals. Consequently, they had
to meet unforeseen needs for joint actions by inventing
communicative actions to achieve coordination on the spot.
Since professional teams are generally able to anticipate what
will come next, they are also able to coordinate their work
more effectively. That new teams perform in a less anticipa-
tory fashion than experienced teams was also showed in a
study comparing experienced surgeon teams with newly
qualied teams (Zheng & Swanstro m 2009). Nevertheless,
the ndings in all the settings reveal the critical importance of
the unnoticed and taken for granted methods of coordinating
teamwork.
What is already known about this topic
Poor coordination among resuscitation team members
can compromise patient safety.
In healthcare education, students are seldom trained in
teamwork.
Previous research on effective team coordination has
emphasized the necessity to practice verbal forms of
communication in simulation training.
What this paper adds
Verbal communication is not in itself sufcient for
achieving coordinated actions.
Coordination in resuscitation teams presupposes
communicative actions that involves a combination of
bodily conduct and gestures and verbal communication.
Perceiving other team members bodily movements and
verbal actions is vital in the coordination of
resuscitation teams.
Implications for practice and/or policy
Although verbal communication is essential for effective
coordination, the necessity of non-verbal
communication for successful team coordination should
also be acknowledged.
Simulations offer promising solutions since they give
possibilities for training the entirety of coordinated
actions in teams that would otherwise not be possible.
Non-verbal communication necessary for coordination
should be included in brieng and debrieng sessions in
simulation-based team training.
Research on simulation should focus on how verbal
and non-verbal forms of communication are
intertwined in teamwork and how this can be
systematically trained in simulations for the purpose of
improving patient safety.
S.E. Huseb et al.
2248 2011 Blackwell Publishing Ltd
The results highlight how speech and body language
mutually constitute the prerequisites for joint assessment
and action. Consequently, this is something that needs to be
accounted for in the training of nurses and allied professions.
These ndings differ from previous research on coordination
within teams, which suggests that verbal communication
alone or verbal communication and bodily conduct as
separate entities can explain how coordination is achieved
(Cooper & Wakelam 1999, Xiao and the Lotas Group 2001).
An approach to getting things done by employing verbal
communication alone as presupposed in CRM training (Rall
& Dieckmann 2005) may imply that important aspects of
human action are overlooked and remain seen, but unno-
ticed (Garnkel 1967).
One implication for resuscitation team training suggested
here is the importance of instructors including all aspects of
the communication process to promote the learning of
coordination skills. A second implication is that the contra-
dictory results of previous studies (Cooper & Wakelam 1999,
Xiao and the Lotas Group 2001) on coordination, i.e.
whether verbal or non-verbal communication is more effec-
tive for successful coordination within teams, might be
explained by the dynamic changes in communication modes
related to the development of the ongoing situation, as
illustrated here. Whether verbal communication or gestures
are more effective in emergency care cannot be answered in a
general way, since it depends on how situations develop as a
result of moment-to-moment interactions. A third implica-
tion is that the distinction between explicit and implicit
coordination can be somewhat misleading. Obviously acts
referred to as implicit coordination, such as taking positions,
gesturing and non-directed speech, are essential for explicat-
ing the team members understanding of each others actions
and what to do next.
There are huge differences between the simulator and
human beings. Nevertheless, the present results indicate that
the students treated the mannequin as a legitimate repre-
sentation of a human being and employed communicative
actions to achieve coordination relevant for clinical
practice. It is also apparent that this was not an effect of
the simulator itself, but rather that the perceived relevance
was shaped in and through the interaction between the
participants and with the technical environment. For the
students, the mannequin was not just a plastic doll, but a
sufciently realistic representation of a human being for the
purpose of simulating resuscitation. In the words of
Garnkel (1967, p. vii) they exhibited an accountable
understanding of the cardiac arrest situation and were
engaged in treating the simulation as real for all practical
purposes.
Conclusion
The present study emphasizes the tacit, often taken for
granted aspects of teamwork as essential components of
coordinated action and illustrates how simulation-based
environments give possibilities for training important facets
of teamwork that would not otherwise have been possible.
Moreover, it points to the necessity of including these aspects
in simulation-based team training instructions and debrieng
sessions in nursing education. We suggest that future research
on simulation should not focus on verbal- and non-verbal
communication as separate entities. To further improve
patient safety it is necessary to address how different forms
of communication are intertwined in coordinated action and
how these can be systematically trained by means of
simulations.
Acknowledgements
This research was nancially supported by The Laerdal
Foundation for Acute Medicine. The analytic work has been
carried out in cooperation with The Linnaeus Centre for
Research on Learning Interaction and Mediated Communi-
cation in Contemporary Society (LinCS) in Sweden. We wish
to thank Professor Eldar Sreide (Stavanger University
Hospital, Norway) for his valuable contribution to the study
and Erica Johnson, PhD, MPhil (University of Gothenburg,
Sweden) and Peter Dieckmann, PhD, Dipl.-Psych. (Danish
Institute for Medical Simulation, Denmark) for thoughtful
and valuable comments on earlier versions of the manuscript.
Funding
This research received no specic grant from any funding
agency in the public, commercial, or not-for-prot sectors.
Conict of interest
No conict of interest has been declared by the authors.
Author contributions
SEH, HR and FF were responsible for the study conception
and design. SEH performed the data collection. SEH, HR and
FF performed the data analysis. SEH, HR and FF were
responsible for the drafting of the manuscript. SEH, HR and
FF made critical revisions to the paper for important
intellectual content. SEH obtained funding. SEH gave
administrative, technical or material support. HR and FF
supervised the study.
JAN: ORIGINAL RESEARCH Educating for teamwork
2011 Blackwell Publishing Ltd 2249
References
Anderson A. (2008) Team building and simulation. In Manual of
Simulation in Healthcare (Riley R.H., ed.), OUP Oxford, Oxford,
pp. 199211.
Cooper S. & Wakelam A. (1999) Leadership of resuscitation teams:
lighthouse leadership. Resuscitation 42(1), 2745.
Dieckmann P. (ed.) (2009) Using Simulations for Education,
Training and Research. Pabst Science Publisher, Lengerich.
Entin E.E. & Serfaty D. (1999) Adaptive team coordination. Human
Factors 41(2), 312325.
Flanagan B., Nestel D. & Joseph M. (2004) Making patient safety the
focus: crisis resource management in the undergraduate curricu-
lum. Medical Education 38, 5666.
Fritz P.Z., Gray T. & Flanagan B. (2008) Review of mannequin-
based high-fidelity simulation in emergency medicine. Emergency
Medicine Australasia 20, 19.
Garfinkel H. (1967) Studies in Ethnomethodology. Prentice-Hall,
Englewood Cliffs, NJ.
Goodwin C. (2000) Action and embodiment within situated human
interaction. Journal of Pragmatics 32(10), 14891522.
Grote G., Zala-Mezo E. & Grommes P. (2004) The effects of dif-
ferent forms of co-ordination on coping with workload. In Group
Interaction in High Risk Environments (Dietrich R. & Childress
T.M., eds), Ashgate, Aldershot, pp. 3954.
Handley A.J., Koster R., Monsieurs K., Perkins G.D., Davies S. &
Bossaert L. (2005) European Resuscitation Council Guidelines for
Resuscitation 2005. Section 2. Adult basic life support and use of
automated external defibrillators. Resuscitation 67S(1), S7S23.
Heath C. & Luff P. (1992) Collaboration and control-crisis man-
agement and multimedia technology in London underground line
control rooms. Computer Supported Cooperative Work 1(1),
6994.
Heath C. & Luff P. (2000) Technology in Action. Cambridge
University Press, Cambridge.
Heath C., Hindmarsh J. & Luff P. (2010). Video in Qualitative
Research. Analysing Social Interaction in Everyday Life. Sage,
Los Angeles.
Hindmarsh J. & Pilnick A. (2002) The tacit order of teamwork:
collaboration and embodied conduct in anesthesia. Sociological
Quarterly 43, 139164.
Hindmarsh J. & Pilnick A. (2007) Knowing bodies at work:
embodiment and ephemeral teamwork in anaesthesia. Organiza-
tion Studies 28, 13951416.
Jordan B. & Henderson A. (1995) Interaction analysis: foundations
and practice. Journal of the Learning Sciences 4(1), 39103.
Kendon A. (1990) Conducting Interaction: Patterns of Behavior in
Focused Encounters. Cambridge University Press, Cambridge.
Kohn L.T., Corrigan J. & Donaldson M.S. (2000) To Err is Human:
Building a Safer Health System. National Academy Press,
Washington.
Krippendorff K. (2004) Content Analysis: An Introduction to its
Methodology. Sage, Thousand Oaks, CA.
Kyrkjeb J.M., Bratteb G. & Smith-Strm H. (2006) Improving
patient safety by using interprofessional simulation training in
health professional education. Journal of Interprofessional Care
20, 507516.
Manser T., Howard S.K. & Gaba D.M. (2008) Adaptive coordina-
tion in cardiac anaesthesia: a study of situational changes in
coordination patterns using a new observation system. Ergonomics
51, 11531178.
McConaughey E. (2008) Crew resource management in healthcare.
Journal of Perinatal & Neonatal Nursing 22(2), 96104.
Medley C.F. & Horne C. (2005) Using simulation technology for
undergraduate nursing education. The Journal of Nursing Educa-
tion 44(1), 3134.
Polit D. & Beck C.T. (2010) Essentials of Nursing Research:
Appraising Evidence for Nursing Practice. Wolters Kluwer/
Lippincott Williams & Wilkins, Philadelphia.
Rall M. & Dieckmann P. (2005) Simulation and patient safety: the
use of simulation to enhance patient safety on a system level.
Current Anaesthesia & Critical Care 15(5), 273281.
Rall M. & Gaba D. (2005) Patient simulators. In Millers Anesthesia
(Miller R.D., ed.), Elsevier, Philadelphia, pp. 30733103.
Rykenes K. & Larsen T. (2010) The relationship between nursing
students mathematics ability and their performance in a drug
calculation test. Nurse Education Today 30, 697701.
Salas E. & Cannon-Bowers J.A. (2001) The science of training:
a decade of progress. Annual Review of Psychology 52(1),
471499.
Salas E., Wilson K.A., Burke C.S. & Wightman D.C. (2006) Does
crew resource management training work? An update, an exten-
sion, and some critical needs. Human Factors 48, 392412.
Salas E., Wilson K.A., Murphy C.E., King H. & Salisbury M. (2008)
Communicating, coordinating, and cooperating when lives depend
on it: tips for teamwork. Joint Commission Journal on Quality &
Patient Safety 34(6), 333341.
Schegloff E.A. (1998) Body torque. Social Research 65(3), 536596.
Serfaty D., Entin E.E. & Volpe C. (1993) Adaption to Stress in Team
Decision-making and Coordination. Paper presented at the Pro-
ceedings of the Human Factors and Ergonomics Society 37th
Annual Meeting, Human Factors and Ergonomics Society, Santa
Monica, California.
Tschan F., Semmer N.K., Gautschi D., Hunziker P., Spychiger M. &
Marsch S.U. (2006) Leading to recovery: group performance and
coordinative activities in medical emergency driven groups.
Human Performance 19, 277304.
Wittenbaum M.G., Vaugham I.S. & Stasser G. (1998) Coordination
in task-performing groups. In Theory and Research on Small
Groups (Tindale R.S., ed.), Plenum Press, New York, pp. 177
204.
Xiao Y. and the Lotas Group (2001) Understanding coordination in a
dynamic medical environment: methods and results. In New
Trends in Cooperative Activities: Understanding System Dynamics
in Complex Environments (Endsley M.R., McNeese M. & Salas
E., eds), Human Factors and Ergonomics Society, Santa Monica,
CA, pp. 242258.
Zheng B. & Swanstro m L.L. (2009) Videoanalysis of anticipatory
movements performed by surgeons during laparoscopic proce-
dures. Surgical Endoscopy 23(7), 14941498.
S.E. Huseb et al.
2250 2011 Blackwell Publishing Ltd
Appendix 1. A full list of categories and numbers including examples of all communication modes in all
phases and groups
Category Stating unconsciousness
Subcategories Codes and numbers Examples*
Verbal communication Verbal communication
Joint assessment Naming the patient 25 Nora, Nora
Questioning the patient for response 12 Nora, Nora is everything okay
with you?
Validating fellow student (unconsciousness) 3 Yes, she is unconscious
Asking for response and answering no response 1 Nora, Nora, are you awake? No,
we dont get
Asking fellow students for respiration status 2 Is she breathing?
Describing respiration 1 Her breathing is very shallow
Stating absence of pulse 3 There is no pulse
Stating absence of breathing 8 She is not breathing
Stating cardiac arrest 10 Now its cardiac arrest
Fellow student conrming absence of breathing 1 Right, she is not breathing
Questioning is it cardiac arrest 1 Is it cardiac arrest?
Joint action Directive 7 Hallo, get the emergency suitcase
Directive to fellow student 2 Get the heart board
Directive to call 113 1 Will you call 113?
Stating to call 113 1 Ill call 113
Non-verbal
communication
Non-verbal communication
Joint assessment Shaking the mannequin 5 One student shakes the mannequin
(for response)
Looking at fellow student 8 One student looks at a fellow
student and gives an assessment
Touching the mannequin 6 One student touches the
mannequins shoulder
(for response)
Monitoring blood pressure 1 One student puts the blood
pressure monitor on the
mannequins arm
Sensing chest heaves 16 One student (bends down), looks
and listen for chest heaves
Sensing pulse 3 One student puts two ngers on
artery radialis
Bending 17 One student bends down (to look
and listen for chest heaves)
Joint action Looking at fellow students 7 One student looks at a fellow
student and asks a question
Interplay between
verbal and
non-verbal
communication
Interplay between verbal and non-verbal
communication
Joint assessment Naming and touching the mannequin 15 Nora, Nora and touches the
mannequins shoulder
Naming and shaking the mannequin 5 Nora, Nora and shakes the
mannequins shoulders
Asking the patient and sensing response 6 Nora are you here? and touches
the mannequins chin
JAN: ORIGINAL RESEARCH Educating for teamwork
2011 Blackwell Publishing Ltd 2251
Appendix 1. (Continued)
Subcategories Codes and numbers Examples*
Naming and lifting the head and looking 1 Nora, and looks and lifts the
mannequins head
Stating lack of pulse and sensing 3 There is no pulse and puts two
ngers on the artery radialis
Joint action Stating absence of breathing and fast moving 1 She is not breathing and runs for
the door
Stating absence of breathing and sensing 2 She is not breathing, looks and
listens for chest heaves
Stating cardiac arrest and glancing at the two fellow
students
2 Now it is cardiac arrest and looks
at fellow student
Stating cardiac arrest and sensing 2 It is cardiac arrest, cardiac arrest
and puts her hand on the
mannequins chest
Asking whether cardiac arrest has occurred, looking
up and body movements
5 Is it cardiac arrest?, looks at
fellow students, turns around and
goes to the door
Conrming cardiac arrest and sensing chest heaves 1 Yes, it is cardiac arrest and puts
her hand on the mannequins
chest
Verbal statement of calling 113 and doing it 1 I will call 113 for help and picks
up the phone
Directing and looking at fellow student 2 Can you monitor the blood
pressure and looks at fellow
student
Category Preparing for resuscitation
Subcategories Codes and numbers Examples*
Verbal
communication
Verbal communication
Joint action Directing 4 Can you run and get the emergency suitcase
Instructing fellow student to
lay down the back rest
1 Lets see
Joint assessment Repeating naming the patient 1 Nora, Nora
Questioning about respiration 1 Is she still breathing?
Stating absence of breathing 3 She is not breathing, she is not breathing normally
Non-verbal
communication
Non-verbal communication
Joint action Bending down the backrest 24 Two students bend down the back rest so the bed is
in a prone position
Removal of pillows 18 Two students remove the pillows from under the
mannequins head and put them on the table
Doing movements simultaneously 15 Two students lift up the mannequin and remove
the pillows
Orientation to each
other
6 Two students stand opposite to
each other, ready to act
simultaneously
Placing and
removing/moving/fasten
artefacts
8 One student moves the bed
table/moves the head
board and places it on the oor
S.E. Huseb et al.
2252 2011 Blackwell Publishing Ltd
Appendix 1. (Continued)
Subcategories Codes and numbers Examples*
Moves to give another
space
16 One student moves to remove
the headboard and fellow
student changes position
Looking at fellow students 12 One student looks at fellow
students to synchronize
actions
Interplay between
verbal and
non-verbal
communication
Interplay between verbal and non-verbal communi-
cation
Joint action Directing and looking 1 Can you run and get the emergency
suitcase and looks at fellow student
Directing and moving 3 Lets see and student 1 helps student
2 to lay down the back rest
Joint assessment Stating absence of breathing and
sensing and touching the patient
1 She is not breathing, she is not
breathing normally and senses chest
heaves with the hand
Stating absence of breathing
and gazing
1 She is not breathing, she is not
breathing normally and looks at
fellow student
Category Initiating resuscitation
Subcategories Codes and numbers Examples*
Verbal communication Verbal communication
Joint action Directive to call 113 15 Will you call 113?
Directive to start compressions 15 Will you start compressions?
Directive to remove the headboard 15 Remove the headboard
Directive to start ventilation 15 Can you give some blows?
Stating start of compressions 5 Ill start compressions
Asking to call the physician 1 Should we call the physician?
Asking for medical device 2 Will you pick up the mask for me?
Asking to open the patients mouth 1 Can you open the mouth so I can put in the
oral airway?
Naming artefacts 1 Heart board
Stating to go and get medical devices 3 Ill go and get the heart board, AED and
emergency suitcase
Correcting behaviour (give injection) 1 You dont need to give the injection now
Joint assessment Stating cardiac arrest 2 Shes in cardiac arrest
Validating cardiac arrest 1 Yes, I think we have a cardiac arrest here
Asking to give information 7 What did the physician say about the treatment
Answering what was said about the
patients status
1 The physician will arrive in ten minutes
Non-verbal
communication
Non-verbal communication
JAN: ORIGINAL RESEARCH Educating for teamwork
2011 Blackwell Publishing Ltd 2253
Appendix 1. (Continued)
Subcategories Codes and numbers Examples*
Joint action Body movements to get artefacts 15 One student moves around the bed
to get the heart board
Pointing at artefacts 4 One student speaks in the phone and points at the
AED
Synchronic body movements 6 Two students lifts up the mannequin to place the
heart board
Placing artefacts 1 One student moves the breakfast tray from the bed
table to the desk
Collecting and placing artefacts 4 One student removes the emergency suitcase and
AED from the oor to the desk
Lifting the mannequin and placing
headboards
1 Two students lift the mannequin and the third
student places the headboard under its chest area
Changes of body position, turning
head and torso
5 One student turns her head and torso towards fellow
students while speaking into the phone: we have a
cardiac arrest here
Body moves and showing artefacts 3 One student moves from the desk to the bed, holding
a syringe in her hand
Taps fellow student and hand over
the oral airway
1 One student talks into the phone while he picks up
the oral airway and taps a fellow student
Grab fellow students arm 1 One student grabs fellow students arm
Anticipating each others actions 7 One student picks up the bag-mask with one hand.
Seeing this action, a fellow student lifts the
mannequins head and removes the pillows with
her other hand
Looking at fellow students 18 One student speaks into the phone and looks at a
fellow student
Joint assessment Sensing 3 One student puts her hand on the mannequins chest
Listening, looking and sensing 1 One student bends down, looks, listens and uses her
senses to detect chest heaves
Interplay between verbal and
non-verbal communication
Interplay between verbal and non-verbal communi-
cation
Joint action Directing and moving headboard
while moving bodies
7 Help me lift her up. Fellow student lifts up the
mannequin and places the head board under the
mannequin
Directing, looking and pointing 11 You must connect the oxygen and looks at fellow
student, moves his eyes to the oxygen device, and
points at it
Directing action and body movements 1 Heart board and bends down, grabbing the heart
board
Directing and gripping fellow students arm 1 You start doing compressions and grabs fellow
students arm
Directives to call and tapping, gives the oral
airway to fellow student
1 Put it down (the AED) and picks up the oral airway
and taps fellow student on the shoulder and hands
over the airway
Stating not to inject medication and looking
at fellow student
2 I dont think I should give the injection now and
gazes at fellow student
Statements (bring AED) and body movements 2 Yes, Ill go and pick up the medical devices and
goes to the door
Asking about information and body movements 2 What did they say (on the phone)? and turns
around to pick up the AED
Naming the oral airway/head board and looking
and/or pointing/sensing/body movements
19 The oral airway and points at the oral airway on
the desk, looking at fellow student
S.E. Huseb et al.
2254 2011 Blackwell Publishing Ltd
Appendix 1. (Continued)
Subcategories Codes and numbers Examples*
Stating what it is,
its purpose and
demonstrating
1 Heres a syringe with Apran (Metoclopramide), Ill
give it intramuscular and moves from the desk to
the bed, holding a syringe in her hand
Joint assessment Stating and sensing lack of
chest heaves
2 It doesnt feel like shes breathing and holding one
hand on the mannequins chest
Stating cardiac arrest,
looking and
receiving artefacts
1 Its cardiac arrest and looks at fellow student, who
hands over the head board
Conrming cardiac arrest
and body movements,
removing artefacts
19 No life signs and moves behind the bed and
removes the headboard
*The author has tried to give non-ambiguous examples for each sub categories. However, depending on the context, the reader imagines a
statement might fall into different subcategories.
The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientic journal. JAN contributes to the advancement of
evidence-based nursing, midwifery and health care by disseminating high quality research and scholarship of contemporary relevance
and with potential to advance knowledge for practice, education, management or policy. JAN publishes research reviews, original
research reports and methodological and theoretical papers.
For further information, please visit JAN on the Wiley Online Library website: www.wileyonlinelibrary.com/journal/jan
Reasons to publish your work in JAN:
High-impact forum: the worlds most cited nursing journal and with an Impact Factor of 1540 ranked 9th of 85 in the 2010
Thomson Reuters Journal Citation Report (Social Science Nursing). JAN has been in the top ten every year for a decade.
Most read nursing journal in the world: over 3 million articles downloaded online per year and accessible in over 10,000 libraries
worldwide (including over 6,000 in developing countries with free or low cost access).
Fast and easy online submission: online submission at http://mc.manuscriptcentral.com/jan.
Positive publishing experience: rapid double-blind peer review with constructive feedback.
Early View: rapid online publication (with doi for referencing) for accepted articles in nal form, and fully citable.
Faster print publication than most competitor journals: as quickly as four months after acceptance, rarely longer than seven months.
Online Open: the option to pay to make your article freely and openly accessible to non-subscribers upon publication on Wiley
Online Library, as well as the option to deposit the article in your own or your funding agencys preferred archive (e.g. PubMed).
JAN: ORIGINAL RESEARCH Educating for teamwork
2011 Blackwell Publishing Ltd 2255
This document is a scanned copy of a printed document. No warranty is given about the accuracy of the copy.
Users should refer to the original published version of the material.
Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- SwitchwordDocument17 pagesSwitchwordnaya17817100% (2)
- Sanskrit Vol1Document203 pagesSanskrit Vol1ngc1729100% (7)
- Darfting and Pleading SlidesDocument29 pagesDarfting and Pleading Slidesbik11111Pas encore d'évaluation
- Armstrong, Isobel - Novel Politics - Democratic Imaginations in Nineteenth-Century Fiction PDFDocument298 pagesArmstrong, Isobel - Novel Politics - Democratic Imaginations in Nineteenth-Century Fiction PDFNones Noneach100% (2)
- Propositional Logic: If and Only If (Rather Than Plus, Minus, Negative, TimesDocument46 pagesPropositional Logic: If and Only If (Rather Than Plus, Minus, Negative, Timesrams3340% (1)
- The Evolution of Winnicotts ThinkingDocument369 pagesThe Evolution of Winnicotts ThinkingJuan Pedro GaresePas encore d'évaluation
- Competency Training Adolescent Health Service WorkersDocument349 pagesCompetency Training Adolescent Health Service WorkersCha Cha100% (1)
- Organizational EffectivenessDocument29 pagesOrganizational Effectivenessabhishek ibsar100% (2)
- Emma J. Stafford - Greek Cults of Deified AbstractionsDocument269 pagesEmma J. Stafford - Greek Cults of Deified Abstractions21Tauri100% (1)
- Gestalt Therapy Fundamentals in Contemporary ContextDocument24 pagesGestalt Therapy Fundamentals in Contemporary ContextVeronicaPas encore d'évaluation
- Film Text AnalysisDocument81 pagesFilm Text AnalysisKristina SholomPas encore d'évaluation
- Abstract Teacher Education and Professional DevelopmentDocument20 pagesAbstract Teacher Education and Professional Developmentrashbasheer100% (1)
- Even The Rat Was White PDFDocument2 pagesEven The Rat Was White PDFAshley0% (23)
- Critical Reading Skills and TechniquesDocument21 pagesCritical Reading Skills and TechniquesMARIA JAVED BSN-FA20-022100% (1)
- Text Mining Applications and TheoryDocument223 pagesText Mining Applications and TheoryXiangcao Liu100% (4)
- Meds Last NamesDocument1 pageMeds Last NamesChristina BarrettPas encore d'évaluation
- AlzheimerDocument2 pagesAlzheimerChristina BarrettPas encore d'évaluation
- Perspectives of Homeless People On Their Health and HealthcareDocument10 pagesPerspectives of Homeless People On Their Health and HealthcareChristina Barrett100% (1)
- Students Perceptions of IncivilityDocument7 pagesStudents Perceptions of IncivilityChristina BarrettPas encore d'évaluation
- LVN Program Estimated CostsDocument1 pageLVN Program Estimated CostsChristina BarrettPas encore d'évaluation
- DNA ArticleDocument5 pagesDNA ArticleChristina BarrettPas encore d'évaluation
- Nursing Attitudes Toward Information TechnologyDocument8 pagesNursing Attitudes Toward Information TechnologyChristina BarrettPas encore d'évaluation
- The Health and Psychosocial Burden of of Alcohol AbuseDocument4 pagesThe Health and Psychosocial Burden of of Alcohol AbuseChristina BarrettPas encore d'évaluation
- Ways To Remember Medications CardiacDocument2 pagesWays To Remember Medications CardiacChristina BarrettPas encore d'évaluation
- Meds Last NamesDocument1 pageMeds Last NamesChristina BarrettPas encore d'évaluation
- Meds Last NamesDocument1 pageMeds Last NamesChristina BarrettPas encore d'évaluation
- False MemoryDocument6 pagesFalse MemoryCrazy BryPas encore d'évaluation
- To 2 YearsDocument16 pagesTo 2 YearsEli Rguez CasillasPas encore d'évaluation
- Improve subject-verb agreement skillsDocument6 pagesImprove subject-verb agreement skillsOjje Fauzi Hukum67% (3)
- APMF Submission to Inquiry into Definition of CharitiesDocument18 pagesAPMF Submission to Inquiry into Definition of CharitiesBhaktha SinghPas encore d'évaluation
- The Islamic MemeplexDocument3 pagesThe Islamic MemeplexSaif RahmanPas encore d'évaluation
- Bailey Et Al. 2016. Using A Narrative Approach To Understand Place AttachmentsDocument12 pagesBailey Et Al. 2016. Using A Narrative Approach To Understand Place AttachmentsNatalia MolinaPas encore d'évaluation
- A Guide To Writing SubmissionsDocument10 pagesA Guide To Writing SubmissionsELIJAH M. OMBEOPas encore d'évaluation
- BUS3110M Strategic Management Individual AssignmentDocument5 pagesBUS3110M Strategic Management Individual Assignmentprojectwork185Pas encore d'évaluation
- Notes On AffixDocument6 pagesNotes On Affixrenata kristiPas encore d'évaluation
- Chapter I The Self From Various PersDocument45 pagesChapter I The Self From Various PersMavyPas encore d'évaluation
- Why can't we see objects in the darkDocument4 pagesWhy can't we see objects in the darkJATIPas encore d'évaluation
- Argumentative-Essay CounterargumentDocument2 pagesArgumentative-Essay CounterargumentVũ ĐỗPas encore d'évaluation
- Astha Koota Matching HoroscopesDocument4 pagesAstha Koota Matching HoroscopesastrosanthoshPas encore d'évaluation
- The Language of Paradox in The Ironic Poetry of Emily DickinsonDocument16 pagesThe Language of Paradox in The Ironic Poetry of Emily DickinsonTanishq KambojPas encore d'évaluation
- A Day On The Grand Canal With The Emperor of ChinaDocument2 pagesA Day On The Grand Canal With The Emperor of ChinaÇağrı KoçPas encore d'évaluation