Vous aimerez peut-être aussi
- ICD-10 Codes Used To Identify Adverse Drug Events in Administrative Data: A Systematic ReviewDocument11 pagesICD-10 Codes Used To Identify Adverse Drug Events in Administrative Data: A Systematic Reviewleniamelia14Pas encore d'évaluation
- Using: ComputerizedDocument5 pagesUsing: ComputerizedFebri RizaPas encore d'évaluation
- Research ArticleDocument9 pagesResearch Articlecindy herreraPas encore d'évaluation
- Arshita Matta - 0011 - Assign 2 - Classification of Mental DisorderDocument3 pagesArshita Matta - 0011 - Assign 2 - Classification of Mental DisorderArshita MattaPas encore d'évaluation
- Comparison of Mayo Clinic Coding SystemsDocument26 pagesComparison of Mayo Clinic Coding SystemsTan SriPas encore d'évaluation
- Literature Review On Clinical Decision Support System Reducing Medical ErrorDocument7 pagesLiterature Review On Clinical Decision Support System Reducing Medical Errorgvzwyd4nPas encore d'évaluation
- Disease Prediction Using Machine Learning: December 2020Document5 pagesDisease Prediction Using Machine Learning: December 2020Ya'u NuhuPas encore d'évaluation
- Disease Prediction Using Machine LearningDocument5 pagesDisease Prediction Using Machine Learningyashsinghal325Pas encore d'évaluation
- Machine Learning-Based Identification and Rule-Based Normalization of Adverse Drug Reactions in Drug LabelsDocument9 pagesMachine Learning-Based Identification and Rule-Based Normalization of Adverse Drug Reactions in Drug LabelsArmanPas encore d'évaluation
- Application of Deep Learning For Early Detection of Covid 19 Using CT Scan ImagesDocument8 pagesApplication of Deep Learning For Early Detection of Covid 19 Using CT Scan ImagesResearch ParkPas encore d'évaluation
- Jamia: OriginalDocument11 pagesJamia: OriginalReroll GenshinPas encore d'évaluation
- From Big Data To Bedside Decision-Making: The Case For AdverseEventsDocument2 pagesFrom Big Data To Bedside Decision-Making: The Case For AdverseEventsDrugs & Therapy StudiesPas encore d'évaluation
- CCD Case StudyDocument5 pagesCCD Case StudyMeenalPas encore d'évaluation
- Drug-Related Admissions and Hospital-Acquired Adverse Drug Events in Germany: A Longitudinal Analysis From 2003 To 2007 of ICD-10-coded Routine DataDocument9 pagesDrug-Related Admissions and Hospital-Acquired Adverse Drug Events in Germany: A Longitudinal Analysis From 2003 To 2007 of ICD-10-coded Routine DataYuli CartrinaPas encore d'évaluation
- A Disease Prediction by Machine Learning Over Bigdata From Healthcare CommunitiesDocument3 pagesA Disease Prediction by Machine Learning Over Bigdata From Healthcare CommunitiesHarikrishnan ShunmugamPas encore d'évaluation
- Data Mining and Knowledge Discovery: Applications, Techniques, Challenges and Process Models in HealthcareDocument7 pagesData Mining and Knowledge Discovery: Applications, Techniques, Challenges and Process Models in Healthcareraj1o1oPas encore d'évaluation
- Evolution and Challenges of EMRDocument3 pagesEvolution and Challenges of EMRAsmamaw K.Pas encore d'évaluation
- JPS Ferranti Cognos SurveillanceDocument7 pagesJPS Ferranti Cognos SurveillancesamlenciPas encore d'évaluation
- PIIS0190962218306649Document1 pagePIIS0190962218306649testPas encore d'évaluation
- An Enhancement in Relevance Knowledge Discovery Model For Medical Reasoning Using CBRMDocument6 pagesAn Enhancement in Relevance Knowledge Discovery Model For Medical Reasoning Using CBRMIjarcet JournalPas encore d'évaluation
- Jurnal KesehatanDocument8 pagesJurnal KesehatanwildaPas encore d'évaluation
- 2022 V13i12025Document5 pages2022 V13i12025kmp pssrPas encore d'évaluation
- A Class Based Approach For Medical Classification of Chest PainDocument5 pagesA Class Based Approach For Medical Classification of Chest Painsurendiran123Pas encore d'évaluation
- (IJCST-V10I5P13) :mrs R Jhansi Rani, K Prem Kumar ReddyDocument7 pages(IJCST-V10I5P13) :mrs R Jhansi Rani, K Prem Kumar ReddyEighthSenseGroupPas encore d'évaluation
- Patient Similarity Analytics For Explainable CliniDocument19 pagesPatient Similarity Analytics For Explainable CliniRanjan SatapathyPas encore d'évaluation
- Disease Prediction by Machine Learning Over Big Data From Healthcare CommunitiesDocument3 pagesDisease Prediction by Machine Learning Over Big Data From Healthcare CommunitiesAruna RajPas encore d'évaluation
- Cloud MRM-A Bio-IT Tool For Correlative Studies in Dermatology 30.08.2011Document11 pagesCloud MRM-A Bio-IT Tool For Correlative Studies in Dermatology 30.08.2011Aimoldina AlmaPas encore d'évaluation
- Heart Disease Prediction Using Bio Inspired AlgorithmsDocument7 pagesHeart Disease Prediction Using Bio Inspired Algorithmssanthoshrao19Pas encore d'évaluation
- Predicting Unplanned Hospital Readmissions Using Patient Level DataDocument9 pagesPredicting Unplanned Hospital Readmissions Using Patient Level DataMeetGandhiPas encore d'évaluation
- Identifying Patients With Coronary Microvascular Dysfunction Using Machine LearningDocument7 pagesIdentifying Patients With Coronary Microvascular Dysfunction Using Machine LearningOscar VeraPas encore d'évaluation
- Cheng YFDocument8 pagesCheng YFSutita DaewhaPas encore d'évaluation
- AI in MedicineDocument4 pagesAI in MedicinemjPas encore d'évaluation
- Hcin 543 Database Management m7 Final Report Steven ZhangDocument9 pagesHcin 543 Database Management m7 Final Report Steven Zhangapi-534987967Pas encore d'évaluation
- A S R N L P K M H: Ystematic Eview of Atural Anguage Rocessing For Nowledge Anagement in EalthcareDocument11 pagesA S R N L P K M H: Ystematic Eview of Atural Anguage Rocessing For Nowledge Anagement in EalthcaresuhasiniPas encore d'évaluation
- Chapter Two Literature Review: 2.1 Background Theory of StudyDocument3 pagesChapter Two Literature Review: 2.1 Background Theory of StudyAyinde AbiodunPas encore d'évaluation
- 2022 V13i12025Document5 pages2022 V13i12025kmp pssrPas encore d'évaluation
- Thesis On Electronic Medical RecordsDocument5 pagesThesis On Electronic Medical RecordsPayingSomeoneToWriteAPaperJackson100% (2)
- Chakrabarti Issue 2 Article For WebsiteDocument4 pagesChakrabarti Issue 2 Article For Websiteapi-400507461Pas encore d'évaluation
- Zhan2008 Article CardiacDeviceImplantationInTheDocument7 pagesZhan2008 Article CardiacDeviceImplantationInTheBeto RamirezPas encore d'évaluation
- Health InformaticsDocument10 pagesHealth Informaticsjose layaPas encore d'évaluation
- Design and Implementation of Online Covid-19 Testing: KeywordsDocument6 pagesDesign and Implementation of Online Covid-19 Testing: KeywordslekanPas encore d'évaluation
- Microsoft Word - Paper 2021 PDFDocument4 pagesMicrosoft Word - Paper 2021 PDFSumati BaralPas encore d'évaluation
- Test Bank For Principles of Healthcare Reimbursement 5th Edition by CastoDocument25 pagesTest Bank For Principles of Healthcare Reimbursement 5th Edition by Castoevanmunozdijapqtrbw100% (20)
- Inter-Patient Distance Metrics Using SNOMED CT Defining RelationshipsDocument9 pagesInter-Patient Distance Metrics Using SNOMED CT Defining RelationshipsFebri RizaPas encore d'évaluation
- Ophthalmic Artery Doppler in The Complementary Diagnosis of Preeclampsia: A Systematic Review and Meta-AnalysisDocument11 pagesOphthalmic Artery Doppler in The Complementary Diagnosis of Preeclampsia: A Systematic Review and Meta-AnalysisValia ChuchonPas encore d'évaluation
- Clinical Decision Support SystemsDocument8 pagesClinical Decision Support SystemsPushpendra ChauhanPas encore d'évaluation
- Aspects of Clinical Decision Support SystemsDocument6 pagesAspects of Clinical Decision Support SystemslinfanluntanPas encore d'évaluation
- Disease Prediction Using Machine Learning Algorithms KNN and CNNDocument7 pagesDisease Prediction Using Machine Learning Algorithms KNN and CNNIJRASETPublications100% (1)
- Diabeticratinography - Research PapersDocument18 pagesDiabeticratinography - Research Papersec engineeringPas encore d'évaluation
- Literature Review Early Warning ScoresDocument8 pagesLiterature Review Early Warning Scoresaflsjizaf100% (1)
- Covid 19 Health Prediction Using Supervised Learning With OptimizationDocument5 pagesCovid 19 Health Prediction Using Supervised Learning With OptimizationEditor IJTSRDPas encore d'évaluation
- 6577-Article Text-11782-1-10-20210530Document10 pages6577-Article Text-11782-1-10-20210530Nadia AzriPas encore d'évaluation
- The Role of Radiology in Diagnostic Error: A Medical Malpractice Claims ReviewDocument7 pagesThe Role of Radiology in Diagnostic Error: A Medical Malpractice Claims ReviewEva HikmahPas encore d'évaluation
- Clinical Decision Support System: Fundamentals and ApplicationsD'EverandClinical Decision Support System: Fundamentals and ApplicationsPas encore d'évaluation
- Improved Association Rule For Classification of Type - 2 Diabetic PatientsDocument7 pagesImproved Association Rule For Classification of Type - 2 Diabetic Patientssurendiran123Pas encore d'évaluation
- Comp9 Unit4b Audio TranscriptDocument9 pagesComp9 Unit4b Audio TranscriptP D SpencerPas encore d'évaluation
- Patient Safety Thesis PDFDocument6 pagesPatient Safety Thesis PDFasiagroverprovo100% (2)
- Intelligent Diagnosis With Chinese Electronic Medical Records Based On Convolutional Neural NetworksDocument12 pagesIntelligent Diagnosis With Chinese Electronic Medical Records Based On Convolutional Neural NetworksHardadi Nur AzizPas encore d'évaluation
- Disease Prediction Using Machine Learning Over Big DataDocument8 pagesDisease Prediction Using Machine Learning Over Big Datacaijjournal2Pas encore d'évaluation
- Predictive Analytics Healthcare Clinical PracticeDocument3 pagesPredictive Analytics Healthcare Clinical PracticelauPas encore d'évaluation
- PMMVYDocument12 pagesPMMVYRitesh KumarPas encore d'évaluation
- Interview QuestionsDocument7 pagesInterview QuestionsRitesh KumarPas encore d'évaluation
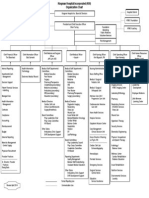
- KHI Organizational Chart 4-14Document1 pageKHI Organizational Chart 4-14Ritesh KumarPas encore d'évaluation
- 3rs Final RuleDocument19 pages3rs Final RuleRitesh KumarPas encore d'évaluation
- 1202 6599v1Document9 pages1202 6599v1Ritesh KumarPas encore d'évaluation
- Improved Accuracy of CodingDocument2 pagesImproved Accuracy of CodingRitesh KumarPas encore d'évaluation
- Texoma Case Study FinalDocument2 pagesTexoma Case Study FinalRitesh KumarPas encore d'évaluation
- APP EMR Prep ArticleDocument12 pagesAPP EMR Prep ArticleRitesh KumarPas encore d'évaluation
- Account Based ResearchDocument1 pageAccount Based ResearchRitesh KumarPas encore d'évaluation
- Account Based ResearchDocument1 pageAccount Based ResearchRitesh KumarPas encore d'évaluation
- 5 Pitfalls of Data MigrationDocument16 pages5 Pitfalls of Data MigrationpameobosoPas encore d'évaluation
- 2010 17210Document66 pages2010 17210Ritesh KumarPas encore d'évaluation
- Role of Incentives RewardsDocument2 pagesRole of Incentives RewardsRitesh KumarPas encore d'évaluation
- Cms CoverageDocument15 pagesCms CoverageRitesh KumarPas encore d'évaluation
- Sales Territory AlignmentDocument0 pageSales Territory AlignmentRitesh KumarPas encore d'évaluation
- Micro Pension For Informal Sector Women WorkersDocument4 pagesMicro Pension For Informal Sector Women WorkersRitesh KumarPas encore d'évaluation
- DownloadDocument6 pagesDownloadRitesh KumarPas encore d'évaluation
- Cms CoverageDocument15 pagesCms CoverageRitesh KumarPas encore d'évaluation
- Akram's ResultDocument1 pageAkram's ResultRitesh KumarPas encore d'évaluation
- Cms CoverageDocument15 pagesCms CoverageRitesh KumarPas encore d'évaluation
- Implementation PlanDocument1 pageImplementation PlanRitesh KumarPas encore d'évaluation
- # College Management/ Principal: 1 Desktop Clock With FlagDocument6 pages# College Management/ Principal: 1 Desktop Clock With FlagRitesh KumarPas encore d'évaluation
- Location - Also See - : 47 A, Near Nehru Vihar Appartment, Road No 2, Nehru Nagar, Pataliputra Colony, Patna - 800013Document3 pagesLocation - Also See - : 47 A, Near Nehru Vihar Appartment, Road No 2, Nehru Nagar, Pataliputra Colony, Patna - 800013Ritesh KumarPas encore d'évaluation
- DNA RepairDocument35 pagesDNA RepairAbid Al RezaPas encore d'évaluation
- COVID-19 Vaccination Certificate from India's Ministry of HealthDocument1 pageCOVID-19 Vaccination Certificate from India's Ministry of Healthbliss bPas encore d'évaluation
- Argumentative EssayDocument7 pagesArgumentative Essayapi-294732914Pas encore d'évaluation
- Practice Exam-10000 SeriesDocument12 pagesPractice Exam-10000 SeriesJuan Romero86% (28)
- LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Document2 pagesLPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Manav ChhabraPas encore d'évaluation
- 2020-68 Annex A - Informed Consent101620Document3 pages2020-68 Annex A - Informed Consent101620roseAngelic ortizPas encore d'évaluation
- PosterDocument3 pagesPosterMadel Tutor ChaturvediPas encore d'évaluation
- Stomach Anatomy in 40 CharactersDocument29 pagesStomach Anatomy in 40 CharactersSupriti Verma Bhatnagar100% (1)
- Nursing Care Plan for Fluid Volume ExcessDocument2 pagesNursing Care Plan for Fluid Volume ExcessUriel CrispinoPas encore d'évaluation
- Unit VII Mental Health and Mental HealthDocument13 pagesUnit VII Mental Health and Mental HealthOmprakash Swami89% (9)
- Patient Information: DateDocument8 pagesPatient Information: Datemehdi chahrour100% (1)
- Glossary of Terms 2nd PartDocument2 pagesGlossary of Terms 2nd Part2DJoyce D.N CapacietePas encore d'évaluation
- Medical Mnemonics 4 PrintDocument65 pagesMedical Mnemonics 4 Printanne0521100% (1)
- Correlation Between Chinese Medicine Constitution and Skin Types: A Study On 187 Japanese WomenDocument6 pagesCorrelation Between Chinese Medicine Constitution and Skin Types: A Study On 187 Japanese Womenthichkhampha_py94Pas encore d'évaluation
- CytologyDocument12 pagesCytologyEsther HutagalungPas encore d'évaluation
- Detoxification of Pesticide Waste Via Activated Carbon Adsorption ProcessDocument11 pagesDetoxification of Pesticide Waste Via Activated Carbon Adsorption ProcessNadia MandasariPas encore d'évaluation
- Johnson & JohnsonDocument13 pagesJohnson & JohnsonShyam SundarPas encore d'évaluation
- ADVANCED BIOCHEMISTRYDocument70 pagesADVANCED BIOCHEMISTRYCik Syin100% (1)
- Nervous System Infections GuideDocument91 pagesNervous System Infections GuideBea Bianca CruzPas encore d'évaluation
- Asepsis and Infection ControlDocument24 pagesAsepsis and Infection Controlabdisalaan hassanPas encore d'évaluation
- The Sense of Stopping Migraine ProphylaxisDocument20 pagesThe Sense of Stopping Migraine ProphylaxisdedeadamPas encore d'évaluation
- Rabipur - (EMC) Print FriendlyDocument8 pagesRabipur - (EMC) Print Friendlyshreyas_chandor3802Pas encore d'évaluation
- Disneynature's Chimpanzee Educator's GuideDocument135 pagesDisneynature's Chimpanzee Educator's GuideNaomi ShapiroPas encore d'évaluation
- Noveon Laser ComparisonDocument20 pagesNoveon Laser ComparisonJohn KenneyPas encore d'évaluation
- JUSTICE BASHEER AHMED SAYEED COLLEGE FOR WOMEN (Autonomous) Chennai 18. S.I.E.T. PILA GLOBOSADocument10 pagesJUSTICE BASHEER AHMED SAYEED COLLEGE FOR WOMEN (Autonomous) Chennai 18. S.I.E.T. PILA GLOBOSAfuture technologyPas encore d'évaluation
- Review on Ayurvedic Concept of Srotas ChannelsDocument4 pagesReview on Ayurvedic Concept of Srotas ChannelsmikikiPas encore d'évaluation
- Masturbation It Might Feel Good But ItsDocument7 pagesMasturbation It Might Feel Good But ItsKshivam KhandelwalPas encore d'évaluation
- Apgar Score 1Document4 pagesApgar Score 1punku1982Pas encore d'évaluation
- Liver Abscess Diagnosis and TreatmentDocument12 pagesLiver Abscess Diagnosis and TreatmentSimon Messi SiringoringoPas encore d'évaluation
- Drill 15 16 Exposition AnalyticalDocument5 pagesDrill 15 16 Exposition AnalyticaliqsanePas encore d'évaluation