Vous aimerez peut-être aussi
- Protection DogsDocument5 pagesProtection Dogsserbi1962Pas encore d'évaluation
- Police DogsDocument8 pagesPolice Dogsserbi1962Pas encore d'évaluation
- The Future of Transnational Litigation: Contemporary Challenges & Solutions For European and Transatlantic LitigationDocument12 pagesThe Future of Transnational Litigation: Contemporary Challenges & Solutions For European and Transatlantic Litigationserbi1962Pas encore d'évaluation
- CCL W Draft Agenda Rev June 42018Document5 pagesCCL W Draft Agenda Rev June 42018serbi1962Pas encore d'évaluation
- Racial ProfilingDocument12 pagesRacial Profilingserbi1962Pas encore d'évaluation
- Public Records Request Submission Form: Login Contact UsDocument2 pagesPublic Records Request Submission Form: Login Contact Usserbi1962Pas encore d'évaluation
- Propst v. McNeil - Arkansas LandlordDocument21 pagesPropst v. McNeil - Arkansas Landlordserbi1962Pas encore d'évaluation
- Villa 2013 CT RF PresentationDocument22 pagesVilla 2013 CT RF Presentationserbi1962Pas encore d'évaluation
- Freight Corridors Concept: ITTS Freight in The Southeast ConferenceDocument17 pagesFreight Corridors Concept: ITTS Freight in The Southeast Conferenceserbi1962Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Ma NuDocument43 pagesMa NuRahul KarnaPas encore d'évaluation
- Legal Ethics ReviewerDocument18 pagesLegal Ethics ReviewerJoel MilanPas encore d'évaluation
- Legal Profession Reviewer MidtermsDocument9 pagesLegal Profession Reviewer MidtermsShasharu Fei-fei LimPas encore d'évaluation
- Crim Soc Set B 2010Document12 pagesCrim Soc Set B 2010Claudine Gubia-on PuyaoPas encore d'évaluation
- Debating: 1. To Order A Sequence of ArgumentsDocument5 pagesDebating: 1. To Order A Sequence of ArgumentspabloPas encore d'évaluation
- C Engleza Scris Var 07Document4 pagesC Engleza Scris Var 07felina07Pas encore d'évaluation
- Easement Act Architecture Module 4 Professional Practice 2 15arc8.4Document17 pagesEasement Act Architecture Module 4 Professional Practice 2 15arc8.4Noothan MPas encore d'évaluation
- PsychopathologyDocument5 pagesPsychopathologyOzzyel CrowleyPas encore d'évaluation
- Social Change ReflectionDocument4 pagesSocial Change Reflectionapi-271193304Pas encore d'évaluation
- Assaf The PhysicianDocument408 pagesAssaf The PhysicianMarla SegolPas encore d'évaluation
- 169375-2014-Bluer Than Blue Joint Ventures Co. v. EstebanDocument9 pages169375-2014-Bluer Than Blue Joint Ventures Co. v. EstebanElimer Teves EspinaPas encore d'évaluation
- Pleasantville:: An Existential Communication JourneyDocument16 pagesPleasantville:: An Existential Communication JourneyFred StevensonPas encore d'évaluation
- Organizational Behavior: Power and PoliticsDocument22 pagesOrganizational Behavior: Power and PoliticsThanh PhươngPas encore d'évaluation
- 2018 Pre Week Bar Lecture in IP TrANSpo and InsuranceDocument14 pages2018 Pre Week Bar Lecture in IP TrANSpo and InsurancemjpjorePas encore d'évaluation
- Grad Nietzsche SyllabusDocument3 pagesGrad Nietzsche SyllabusAnthony CrossPas encore d'évaluation
- Lacan - Mirror Stage - Sheridan PDFDocument5 pagesLacan - Mirror Stage - Sheridan PDFsantanu6Pas encore d'évaluation
- GMRC of A ChristianDocument12 pagesGMRC of A ChristianRaul PostranoPas encore d'évaluation
- Housing Standards Act 2908Document18 pagesHousing Standards Act 2908tarisaiPas encore d'évaluation
- Edu Psy TEXT - (Psychology)Document33 pagesEdu Psy TEXT - (Psychology)Yasmeen JafferPas encore d'évaluation
- Chap. 1 Strategic Vision, Mission and ObjectivesDocument38 pagesChap. 1 Strategic Vision, Mission and ObjectivesOjantaPas encore d'évaluation
- University of The East Basic Education Department-ManilaDocument4 pagesUniversity of The East Basic Education Department-ManilaTrixia ElizanPas encore d'évaluation
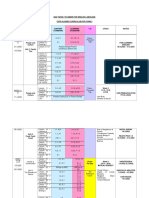
- 2022 Yearly Planner For English LanguageDocument10 pages2022 Yearly Planner For English LanguageAfifah 11Pas encore d'évaluation
- CrimPro Codal Memory Aid FinalsDocument33 pagesCrimPro Codal Memory Aid FinalsMartin EspinosaPas encore d'évaluation
- Time As An Essence of ContractsDocument20 pagesTime As An Essence of ContractsAyushi Agrawal100% (1)
- Systematic DesensitizationDocument10 pagesSystematic Desensitizationxivago7Pas encore d'évaluation
- SPA - SampleDocument2 pagesSPA - SampleAP GeotinaPas encore d'évaluation
- John Marrin Paper 105 Unformatted - Concurrent Delay Revisited - 21 5 12Document16 pagesJohn Marrin Paper 105 Unformatted - Concurrent Delay Revisited - 21 5 12Anonymous 19hUyemPas encore d'évaluation
- Paralege QUICK-Digests ConsolidatedDocument580 pagesParalege QUICK-Digests ConsolidatedPatrick TanPas encore d'évaluation
- Urbanpromise Honduras: Urbanpromise History Urbanpromise Ministries Started in CamdenDocument1 pageUrbanpromise Honduras: Urbanpromise History Urbanpromise Ministries Started in Camdenapi-67779196Pas encore d'évaluation
- Art 171-172PRCDocument2 pagesArt 171-172PRCDan SilPas encore d'évaluation