Vous aimerez peut-être aussi
- Brachial PlexusDocument4 pagesBrachial PlexussaluniasPas encore d'évaluation
- Anatomy of Brachial Plexus: DR - Sadiq Wadood Siddiqui JR3 Department of AnatomyDocument53 pagesAnatomy of Brachial Plexus: DR - Sadiq Wadood Siddiqui JR3 Department of AnatomySadiq Wadood SiddiquiPas encore d'évaluation
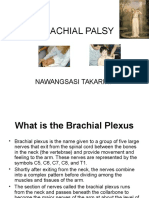
- Brachial Palsy: Nawangsasi TakariniDocument18 pagesBrachial Palsy: Nawangsasi TakariniSatrianianianiPas encore d'évaluation
- PLexo BraquialDocument2 pagesPLexo BraquialSimon Arturo Venancio MasgoPas encore d'évaluation
- Brachial Plexus Block: "Dr. Sami Ur Rehman" House OfficerDocument65 pagesBrachial Plexus Block: "Dr. Sami Ur Rehman" House OfficerSami Ur RehmanPas encore d'évaluation
- Dr. AnanyaDocument55 pagesDr. AnanyatarawifaPas encore d'évaluation
- Brachial PlexusDocument9 pagesBrachial Plexus林耿毅Pas encore d'évaluation
- Anatomy All NotesDocument77 pagesAnatomy All NotesBat ManPas encore d'évaluation
- Brachial PlexusDocument3 pagesBrachial PlexusIshant SinghPas encore d'évaluation
- Brachial Plexus Anatomy: Abdulaziz R. Alanzi Medical Student, Al-Imam University Riyadh, Saudi ArabiaDocument23 pagesBrachial Plexus Anatomy: Abdulaziz R. Alanzi Medical Student, Al-Imam University Riyadh, Saudi ArabiaArybaa MeerPas encore d'évaluation
- Brachial PlexusDocument10 pagesBrachial PlexusPercy Jackson100% (1)
- Key Facts About The Upper Extremity NervesDocument6 pagesKey Facts About The Upper Extremity NervesMetin HakkanPas encore d'évaluation
- Brachial PlexusDocument2 pagesBrachial PlexusemranalshaibaniPas encore d'évaluation
- Dermatomes of The Upper LimbDocument55 pagesDermatomes of The Upper LimbGideon WilliePas encore d'évaluation
- Anatomy Concept Book AtfDocument246 pagesAnatomy Concept Book AtfRishi ShekharPas encore d'évaluation
- Anatomy MSK SAQs AssignmentDocument12 pagesAnatomy MSK SAQs Assignmentaimy.palawataraPas encore d'évaluation
- Anatomy-Ms Respi NeuroDocument10 pagesAnatomy-Ms Respi NeuroImmah PinedaPas encore d'évaluation
- Brachial PlexusDocument7 pagesBrachial PlexusCoco GargaritaPas encore d'évaluation
- Table E-AxillaryDocument18 pagesTable E-Axillaryapi-371785797Pas encore d'évaluation
- Brachial Plexus (Autosaved)Document19 pagesBrachial Plexus (Autosaved)Muhamad SdeqPas encore d'évaluation
- Anatomy - CH 6 & 7Document7 pagesAnatomy - CH 6 & 7cpPas encore d'évaluation
- 1D-19 GRSANA Reviewer 1.04 - Muscles of The Shoulder RegionDocument16 pages1D-19 GRSANA Reviewer 1.04 - Muscles of The Shoulder RegionShaira Aquino VerzosaPas encore d'évaluation
- Brachial PlexusDocument6 pagesBrachial PlexusMuhamad SdeqPas encore d'évaluation
- Ana211 Brachial PlexusDocument8 pagesAna211 Brachial PlexusKalu ComforterPas encore d'évaluation
- Spinal Nerves1Document25 pagesSpinal Nerves1api-19641337Pas encore d'évaluation
- Medianus NerveDocument30 pagesMedianus NerveSammy BudiyantoPas encore d'évaluation
- The Brachial PlexusDocument22 pagesThe Brachial PlexusMusonda LumbwePas encore d'évaluation
- Dr. Syed Irfan Raza ArifDocument27 pagesDr. Syed Irfan Raza ArifSyed Irfan ArifPas encore d'évaluation
- Brachial PlexusDocument24 pagesBrachial Plexusfilza farheenPas encore d'évaluation
- The Brachial Plexus2Document9 pagesThe Brachial Plexus2Dr Tahira NihalPas encore d'évaluation
- Anatomy 06 - Axilla (Pre Med 101)Document8 pagesAnatomy 06 - Axilla (Pre Med 101)Navoda Dulshan PereraPas encore d'évaluation
- Anatomy Concept BookDocument246 pagesAnatomy Concept Bookmusaazi alexPas encore d'évaluation
- Unit4 DM - Vb.inddDocument31 pagesUnit4 DM - Vb.inddAlexPas encore d'évaluation
- Clavicular Head:: RD THDocument3 pagesClavicular Head:: RD THSam PadrePas encore d'évaluation
- Handount Limbs CompleteDocument67 pagesHandount Limbs CompletebigprogrammeramPas encore d'évaluation
- ANAPHY LEC Spinal CordDocument2 pagesANAPHY LEC Spinal CordReigh DakotaPas encore d'évaluation
- Anatomy Nerves of UL 2022Document45 pagesAnatomy Nerves of UL 2022Malak AhmedPas encore d'évaluation
- The Gross Appearance of Spinal Cord-Lec by EmmaDocument32 pagesThe Gross Appearance of Spinal Cord-Lec by EmmaJen Passilan100% (1)
- PTA 20 - Plexi ProjectDocument12 pagesPTA 20 - Plexi ProjectM TnPas encore d'évaluation
- Plexo BraquialDocument7 pagesPlexo BraquialcataPas encore d'évaluation
- Nerves of Upper LimbDocument9 pagesNerves of Upper LimbRaymond PosumaPas encore d'évaluation
- Nervous SystemDocument60 pagesNervous SystemFiraol DiribaPas encore d'évaluation
- Organization of Nervous System - MBBS NewDocument53 pagesOrganization of Nervous System - MBBS NewDorin PathakPas encore d'évaluation
- Braquial PlexusDocument9 pagesBraquial PlexusLaura TapiaPas encore d'évaluation
- Experiment No. 2: The Nervous SystemDocument6 pagesExperiment No. 2: The Nervous SystemmasorPas encore d'évaluation
- Anesthesiology Midterm Ii Spinal and Epidural AnesthesiaDocument8 pagesAnesthesiology Midterm Ii Spinal and Epidural AnesthesiaLeslie Ann Pablo MarantanPas encore d'évaluation
- Terminology List Nervous SysDocument2 pagesTerminology List Nervous SyswinniepichoPas encore d'évaluation
- Anatomy, Imaging and Pathologic Conditions of Brachial PlexusDocument67 pagesAnatomy, Imaging and Pathologic Conditions of Brachial PlexusChrista Levina DaniswaraPas encore d'évaluation
- Muscles of Upper LimbDocument21 pagesMuscles of Upper Limbمحمد علىPas encore d'évaluation
- Cervical, Brachial PlexusDocument31 pagesCervical, Brachial PlexusSophy AhdyPas encore d'évaluation
- Lecture 11 - Nerves of The ForelimbDocument10 pagesLecture 11 - Nerves of The ForelimbAndrew Blessed KatabaPas encore d'évaluation
- Anatomy 3 Upper LimbsDocument5 pagesAnatomy 3 Upper LimbszahraaPas encore d'évaluation
- Neck RegionDocument47 pagesNeck RegionShiela ClementePas encore d'évaluation
- Brachial PlexusDocument62 pagesBrachial PlexusTutankhamoun Akhenatoun100% (2)
- ملخص للعضلاتDocument22 pagesملخص للعضلاتn52p8mhvvbPas encore d'évaluation
- Anatomy Tables SarahDocument4 pagesAnatomy Tables Sarahanasadel1234.1Pas encore d'évaluation
- Clavicular Part: Flexes and Acromial Part: AbductsDocument1 pageClavicular Part: Flexes and Acromial Part: AbductsMihaelaPas encore d'évaluation
- Dash8 200 300 Electrical PDFDocument35 pagesDash8 200 300 Electrical PDFCarina Ramo LakaPas encore d'évaluation
- Ict's - 2022 - Mentorship - Summarized - Thread - by - Trader - Theory - Sep 22, 22 - From - RattibhaDocument11 pagesIct's - 2022 - Mentorship - Summarized - Thread - by - Trader - Theory - Sep 22, 22 - From - RattibhaChristiana OnyinyePas encore d'évaluation
- MMB & DFT 2012 Workshop ProceedingsDocument44 pagesMMB & DFT 2012 Workshop ProceedingsFelipe ToroPas encore d'évaluation
- Teal Motor Co. Vs CFIDocument6 pagesTeal Motor Co. Vs CFIJL A H-DimaculanganPas encore d'évaluation
- Technical DescriptionDocument2 pagesTechnical Descriptioncocis_alexandru04995Pas encore d'évaluation
- LET-English-Structure of English-ExamDocument57 pagesLET-English-Structure of English-ExamMarian Paz E Callo80% (5)
- Beng (Hons) Telecommunications: Cohort: Btel/10B/Ft & Btel/09/FtDocument9 pagesBeng (Hons) Telecommunications: Cohort: Btel/10B/Ft & Btel/09/FtMarcelo BaptistaPas encore d'évaluation
- Sheet (8) Synchronous Machine Problem (1) :: SolutionDocument5 pagesSheet (8) Synchronous Machine Problem (1) :: Solutionمكاريوس عيادPas encore d'évaluation
- 5G NR Essentials Guide From IntelefyDocument15 pages5G NR Essentials Guide From IntelefyUzair KhanPas encore d'évaluation
- USTH Algorithm RecursionDocument73 pagesUSTH Algorithm Recursionnhng2421Pas encore d'évaluation
- Iroquois Clothes and WampumDocument3 pagesIroquois Clothes and Wampumapi-254323856Pas encore d'évaluation
- Measures For FloodsDocument4 pagesMeasures For FloodsMutsitsikoPas encore d'évaluation
- Analysis of MMDR Amendment ActDocument5 pagesAnalysis of MMDR Amendment ActArunabh BhattacharyaPas encore d'évaluation
- Turnbull CV OnlineDocument7 pagesTurnbull CV Onlineapi-294951257Pas encore d'évaluation
- Historical Perspective of OBDocument67 pagesHistorical Perspective of OBabdiweli mohamedPas encore d'évaluation
- Certificate of Attendance: Yosapat NashulahDocument2 pagesCertificate of Attendance: Yosapat NashulahStrata WebPas encore d'évaluation
- Albert-Einstein-Strasse 42a, D-63322 Roedermark, Germany Tel.: 0049 (0) 6074-7286503 - Fax: 0049 (0) 6074-7286504Document19 pagesAlbert-Einstein-Strasse 42a, D-63322 Roedermark, Germany Tel.: 0049 (0) 6074-7286503 - Fax: 0049 (0) 6074-7286504Ilias Asimakis100% (1)
- Manual TV Hyundai HYLED3239iNTMDocument40 pagesManual TV Hyundai HYLED3239iNTMReinaldo TorresPas encore d'évaluation
- Newcastle University Dissertation FormatDocument6 pagesNewcastle University Dissertation FormatWriteMyEnglishPaperForMeSterlingHeights100% (1)
- Hauling AgreementDocument2 pagesHauling AgreementE.A. Francisco Trucking100% (3)
- RADMASTE CAPS Grade 11 Chemistry Learner GuideDocument66 pagesRADMASTE CAPS Grade 11 Chemistry Learner Guideamajobe34Pas encore d'évaluation
- Issue15 - Chirag JiyaniDocument6 pagesIssue15 - Chirag JiyaniDipankar SâháPas encore d'évaluation
- Vtoris 100% Clean Paypal Transfer Guide 2015Document8 pagesVtoris 100% Clean Paypal Transfer Guide 2015Sean FrohmanPas encore d'évaluation
- Course: Introduction To Geomatics (GLS411) Group Practical (2-3 Persons in A Group) Practical #3: Principle and Operation of A LevelDocument3 pagesCourse: Introduction To Geomatics (GLS411) Group Practical (2-3 Persons in A Group) Practical #3: Principle and Operation of A LevelalyafarzanaPas encore d'évaluation
- Review and Basic Principles of PreservationDocument43 pagesReview and Basic Principles of PreservationKarl Marlou Bantaculo100% (1)
- Context in TranslationDocument23 pagesContext in TranslationRaluca FloreaPas encore d'évaluation
- Case Study in Architectural Structures: A-7E Avionics System - ADocument36 pagesCase Study in Architectural Structures: A-7E Avionics System - Ajckz8Pas encore d'évaluation
- Jar Doc 06 Jjarus Sora Executive SummaryDocument3 pagesJar Doc 06 Jjarus Sora Executive Summaryprasenjitdey786Pas encore d'évaluation
- Math ExamDocument21 pagesMath ExamedgemarkPas encore d'évaluation
- YhhjjDocument52 pagesYhhjjSam CunananPas encore d'évaluation