Vous aimerez peut-être aussi
- Anatomy and Physiology - Dengue FeverDocument3 pagesAnatomy and Physiology - Dengue Feverhael yam62% (13)
- SCE Practicaldiabetes - ElzohryDocument107 pagesSCE Practicaldiabetes - ElzohryAE67% (3)
- Non-Cardiac Chest PainDocument5 pagesNon-Cardiac Chest PainRPas encore d'évaluation
- Essential Questions in Paediatrics For MRCPCH v2 PDFDocument208 pagesEssential Questions in Paediatrics For MRCPCH v2 PDFa4aboo100% (11)
- Basic Math Ability Exam A Relias Graded ADocument6 pagesBasic Math Ability Exam A Relias Graded ADebs MaxPas encore d'évaluation
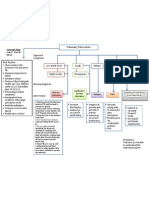
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- Herberg 2014Document8 pagesHerberg 2014ANA HERNÁNDEZPas encore d'évaluation
- Outcome - of - Splenectomy - in - Children - Young20151023 737 1ml8k9i With Cover Page v2Document6 pagesOutcome - of - Splenectomy - in - Children - Young20151023 737 1ml8k9i With Cover Page v2sarahloba100Pas encore d'évaluation
- Cox 2015Document11 pagesCox 2015Julio Orallo MartínezPas encore d'évaluation
- Fop 1Document14 pagesFop 1Ricardo CorreaPas encore d'évaluation
- Tga Lagi PDFDocument4 pagesTga Lagi PDFMYMAPas encore d'évaluation
- Management of T.B.M. Hydrocephalus Role of Shunt Surgery - 55 58Document4 pagesManagement of T.B.M. Hydrocephalus Role of Shunt Surgery - 55 58Kushal BhatiaPas encore d'évaluation
- 2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathyDocument9 pages2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathybanupluPas encore d'évaluation
- Jurnal 15Document5 pagesJurnal 15rifkipspdPas encore d'évaluation
- SN Chez 1984Document6 pagesSN Chez 1984ROHITPas encore d'évaluation
- Viswanathan 2008Document6 pagesViswanathan 2008deepaPas encore d'évaluation
- Tetralogy of FallotDocument5 pagesTetralogy of FallotSaloni MehtaPas encore d'évaluation
- Reading Versola Ventricular TachycardiaDocument3 pagesReading Versola Ventricular TachycardiaRaijenne VersolaPas encore d'évaluation
- Hollehorst PlaquesDocument3 pagesHollehorst PlaquesErick Roa GandicaPas encore d'évaluation
- Lapkas Pediatrik NLDocument31 pagesLapkas Pediatrik NLHannaTashiaClaudiaPas encore d'évaluation
- Modi Fied Blalock Taussig Shunt: A Not-So-Simple Palliative ProcedureDocument7 pagesModi Fied Blalock Taussig Shunt: A Not-So-Simple Palliative ProcedureJakler NichelePas encore d'évaluation
- OperabilityinL RDocument6 pagesOperabilityinL RVimal NishadPas encore d'évaluation
- Aortic Valve Stenosis - Curr. View On Diagnostics, TRTMT - P. Santavy (Intech, 2011) WWDocument156 pagesAortic Valve Stenosis - Curr. View On Diagnostics, TRTMT - P. Santavy (Intech, 2011) WWAnca AndronicPas encore d'évaluation
- Pulmonary EmbolismDocument25 pagesPulmonary EmbolismRaymund VadilPas encore d'évaluation
- Sarcoidosis Review. JAMADocument9 pagesSarcoidosis Review. JAMARafael ReañoPas encore d'évaluation
- Presentacion 2018 Orlando 1111Document24 pagesPresentacion 2018 Orlando 1111José Luis AlonsoPas encore d'évaluation
- Ajc 10018 Review GunerDocument11 pagesAjc 10018 Review GunerMaria Goretty L. TobingPas encore d'évaluation
- Hour Pathophysiologic Approach To The Golden: Review of A Major Pulmonary EmbolismDocument31 pagesHour Pathophysiologic Approach To The Golden: Review of A Major Pulmonary EmbolismSilvio SillitanoPas encore d'évaluation
- 1 s2.0 S0031395503002153 MainDocument21 pages1 s2.0 S0031395503002153 Maindiego bustosPas encore d'évaluation
- Acute Coronary Syndrome inDocument2 pagesAcute Coronary Syndrome inpaul_preda_bvPas encore d'évaluation
- Pulmonary Atresia With Ventricular Septal Defect: Systematic ReviewDocument10 pagesPulmonary Atresia With Ventricular Septal Defect: Systematic ReviewIvan VeriswanPas encore d'évaluation
- Chi Et Al - 2013 - An Update On Pulmonary Complications of Hematopoietic Stem Cell TransplantationDocument10 pagesChi Et Al - 2013 - An Update On Pulmonary Complications of Hematopoietic Stem Cell TransplantationRutvik ShahPas encore d'évaluation
- Cardiogenic Shock: Physical FindingsDocument9 pagesCardiogenic Shock: Physical FindingsEduardo Perez GonzalezPas encore d'évaluation
- Saddle Pulmonary Embolism: A Rare Case of Proximal Pulmonary EmbolismDocument3 pagesSaddle Pulmonary Embolism: A Rare Case of Proximal Pulmonary EmbolismIJAR JOURNALPas encore d'évaluation
- 01-16 Optimal Therapy For Unstable Pulmonar EmbolismDocument4 pages01-16 Optimal Therapy For Unstable Pulmonar EmbolismLesly Peinado TorresPas encore d'évaluation
- Lapkas TOF COMPLETE-1 Edit-2Document61 pagesLapkas TOF COMPLETE-1 Edit-2Dora HasturaPas encore d'évaluation
- Pulmonary Atelectasis: A Pathogenic Perioperative EntityDocument18 pagesPulmonary Atelectasis: A Pathogenic Perioperative Entityハルァン ファ烏山Pas encore d'évaluation
- Acute Myocardial Infarction: Primary Angioplasty: Coronary DiseaseDocument5 pagesAcute Myocardial Infarction: Primary Angioplasty: Coronary DiseaseGuțu SergheiPas encore d'évaluation
- Unusual Cause of Neonatal Cyanosis: Journal of The Saudi Heart AssociationDocument3 pagesUnusual Cause of Neonatal Cyanosis: Journal of The Saudi Heart AssociationfikaPas encore d'évaluation
- Chest 2002 TEP Excelente PDFDocument31 pagesChest 2002 TEP Excelente PDFEdwin AlvarezPas encore d'évaluation
- TEP Systemic Thrombolysis For Pulmonary Embolism Evidence, Patient Selection, and Protocols For ManagementDocument10 pagesTEP Systemic Thrombolysis For Pulmonary Embolism Evidence, Patient Selection, and Protocols For Managementbenitez1228Pas encore d'évaluation
- The Perioperative Complication Rate of Orthopedic PDFDocument10 pagesThe Perioperative Complication Rate of Orthopedic PDFAnh Nguyen HuuPas encore d'évaluation
- An Unusual Case of Polycythemia Vera With A Complication of Pancreatic PseudocystDocument3 pagesAn Unusual Case of Polycythemia Vera With A Complication of Pancreatic PseudocystAgus PrimaPas encore d'évaluation
- Saddle Embolism in The Pulmonary Artery BifurcationDocument3 pagesSaddle Embolism in The Pulmonary Artery BifurcationAtiquzzaman RinkuPas encore d'évaluation
- Joseph 2016 CardioDocument30 pagesJoseph 2016 CardioCarlos Daniel da Silva AlonsoPas encore d'évaluation
- IMP Shock Etiol 5y Outcome VA-ECMO Edit 2023Document3 pagesIMP Shock Etiol 5y Outcome VA-ECMO Edit 2023vladbvs16Pas encore d'évaluation
- Congenital Lobar EmphysemaDocument3 pagesCongenital Lobar Emphysemamadimadi11Pas encore d'évaluation
- C2 U5 Williams Et Al Critical Care Clinics 2013Document32 pagesC2 U5 Williams Et Al Critical Care Clinics 2013Diego CrucesPas encore d'évaluation
- PHTN+Pulmonary Hypertension+CDH+Congenital Diaphragmatic HerniaDocument8 pagesPHTN+Pulmonary Hypertension+CDH+Congenital Diaphragmatic Herniahadi40canadaPas encore d'évaluation
- Pulmonary Stenosis As A Result of Valve Dysplasia Is The Most CommonDocument22 pagesPulmonary Stenosis As A Result of Valve Dysplasia Is The Most CommonFull MarksPas encore d'évaluation
- Contr Over SiaDocument2 pagesContr Over SianaimPas encore d'évaluation
- Buesing 2011 Partial Splenectomy For Hereditary Spherocytosis A Multi-Institutional ReviewDocument6 pagesBuesing 2011 Partial Splenectomy For Hereditary Spherocytosis A Multi-Institutional ReviewBogdan TrandafirPas encore d'évaluation
- Current Management of Infants and Children With Single Ventricle AnatomyDocument13 pagesCurrent Management of Infants and Children With Single Ventricle AnatomyjahangirealamPas encore d'évaluation
- Pulmonary Embolism - European Heart Journal 2012Document12 pagesPulmonary Embolism - European Heart Journal 2012Andreas IoannouPas encore d'évaluation
- 1276 FullDocument4 pages1276 FullRyl WonPas encore d'évaluation
- 01 Cir 15 6 814Document13 pages01 Cir 15 6 814Niarti Ulan SariPas encore d'évaluation
- Content Server 1Document6 pagesContent Server 1Ajeng Permata AnggitasariPas encore d'évaluation
- Alveolar Capillary Dysplasia With Misalignment of The Pulmonary Veins Clinical Histological and Genetic AspectsDocument8 pagesAlveolar Capillary Dysplasia With Misalignment of The Pulmonary Veins Clinical Histological and Genetic AspectsYi linPas encore d'évaluation
- Transfusion-Related Acute Lung Injury: Pearl Toy,, and Ognjen GajicDocument2 pagesTransfusion-Related Acute Lung Injury: Pearl Toy,, and Ognjen GajicMaulana Akbar LubisPas encore d'évaluation
- Surgical Therapy For Necrotizing Pneumonia and Lung Gangrene PDFDocument6 pagesSurgical Therapy For Necrotizing Pneumonia and Lung Gangrene PDFmichael24kPas encore d'évaluation
- NPT El FinalDocument40 pagesNPT El FinalSelma Alonso BuenabadPas encore d'évaluation
- Anglisht 2Document8 pagesAnglisht 2Ejona SuloPas encore d'évaluation
- CDH Modern MXDocument11 pagesCDH Modern MXphobicmdPas encore d'évaluation
- CDH and Pulmonary HypertensionDocument6 pagesCDH and Pulmonary HypertensionStollery SandboxPas encore d'évaluation
- Contemporary Reviews in Cardiovascular Medicine: Cardiogenic ShockDocument32 pagesContemporary Reviews in Cardiovascular Medicine: Cardiogenic ShockSindhuNugrohoMuktiPas encore d'évaluation
- Euthyroid Goiter With and Without Nodules-Diagnosis and TreatmentDocument12 pagesEuthyroid Goiter With and Without Nodules-Diagnosis and TreatmentOkky Winang SaktyawanPas encore d'évaluation
- Human ESM1/Endocan ELISA Kit: Catalog No. EK0752 Size 96T (8×12 Divisible Strips)Document5 pagesHuman ESM1/Endocan ELISA Kit: Catalog No. EK0752 Size 96T (8×12 Divisible Strips)Okky Winang SaktyawanPas encore d'évaluation
- Stsi NefriDocument2 pagesStsi NefriOkky Winang SaktyawanPas encore d'évaluation
- A - Z of Abdominal Radiology: More InformationDocument10 pagesA - Z of Abdominal Radiology: More InformationOkky Winang SaktyawanPas encore d'évaluation
- DiabetesClinicalPaper en 2011Document24 pagesDiabetesClinicalPaper en 2011Okky Winang SaktyawanPas encore d'évaluation
- Introduction NutritionDocument2 pagesIntroduction NutritionOkky Winang SaktyawanPas encore d'évaluation
- Major Minerals Trace ElementsDocument3 pagesMajor Minerals Trace ElementsOkky Winang SaktyawanPas encore d'évaluation
- Deve HatDocument5 pagesDeve HatOkky Winang SaktyawanPas encore d'évaluation
- Journal Pone 0083335 t003Document1 pageJournal Pone 0083335 t003Okky Winang SaktyawanPas encore d'évaluation
- Tirosin KinaseDocument9 pagesTirosin KinaseOkky Winang SaktyawanPas encore d'évaluation
- Open Recruitment: Unissula Medical Academic Club (Umac) Fakultas Kedokteran Unniversitas Islam Sultan Agung SemarangDocument2 pagesOpen Recruitment: Unissula Medical Academic Club (Umac) Fakultas Kedokteran Unniversitas Islam Sultan Agung SemarangOkky Winang SaktyawanPas encore d'évaluation
- Amenorrhea PDFDocument16 pagesAmenorrhea PDFOkky Winang SaktyawanPas encore d'évaluation
- Induction of Cell Cycle Arrest and Apoptosis in Human Breast Cancer Cells by QuercetinDocument1 pageInduction of Cell Cycle Arrest and Apoptosis in Human Breast Cancer Cells by QuercetinOkky Winang SaktyawanPas encore d'évaluation
- A Thirty Five-Year-Old Woman With Acute Febrile Illness, Headache, General Weakness, Muscle Pain, History of SeizureDocument1 pageA Thirty Five-Year-Old Woman With Acute Febrile Illness, Headache, General Weakness, Muscle Pain, History of SeizureOkky Winang SaktyawanPas encore d'évaluation
- Mechanisms, Prevention, and Treatment of Atrial Fibrillation After Cardiac SurgeryDocument9 pagesMechanisms, Prevention, and Treatment of Atrial Fibrillation After Cardiac SurgeryOkky Winang SaktyawanPas encore d'évaluation
- Structural Abnormalities of The Pulmonary Trunk in Tetralogy of Fallot and Potential Clinical ImplicationsDocument8 pagesStructural Abnormalities of The Pulmonary Trunk in Tetralogy of Fallot and Potential Clinical ImplicationsOkky Winang SaktyawanPas encore d'évaluation
- Uji Sitotoksisitas in Vitro Sediaan Jadi BRM (Biological Response Modifier) Terhadap Sel Kanker ServiksDocument7 pagesUji Sitotoksisitas in Vitro Sediaan Jadi BRM (Biological Response Modifier) Terhadap Sel Kanker ServiksOkky Winang SaktyawanPas encore d'évaluation
- IJoC 2010 3 111Document8 pagesIJoC 2010 3 111Okky Winang SaktyawanPas encore d'évaluation
- Vitamin D and Cardiovascular Disease: Time For Large Randomized TrialsDocument3 pagesVitamin D and Cardiovascular Disease: Time For Large Randomized TrialsOkky Winang SaktyawanPas encore d'évaluation
- Lista Preturi Teste Genetice GendiaDocument227 pagesLista Preturi Teste Genetice GendiaMatei FloriPas encore d'évaluation
- Sports DrinksDocument2 pagesSports DrinksMustofaPas encore d'évaluation
- D An Introduction: Physical Medicine and RehabilitationDocument33 pagesD An Introduction: Physical Medicine and RehabilitationChadPas encore d'évaluation
- Hypopyon in Acute Lymphoblastic Leukemia A Case ReportDocument2 pagesHypopyon in Acute Lymphoblastic Leukemia A Case ReportInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Systemic Diseases and The EyeDocument17 pagesSystemic Diseases and The Eyeapi-337689057Pas encore d'évaluation
- Et TR MedDocument99 pagesEt TR MedThe SciencePas encore d'évaluation
- Repair of HydroceleDocument20 pagesRepair of HydroceleNatanael AdiPas encore d'évaluation
- Avian Influenza in ChickensDocument19 pagesAvian Influenza in ChickensShah NawazPas encore d'évaluation
- Castor OilDocument1 pageCastor OilRohan EarnestPas encore d'évaluation
- Hospital Outpatient Prospective Payment System 2019 Updates - Shared1Document112 pagesHospital Outpatient Prospective Payment System 2019 Updates - Shared1Nunya BiznesPas encore d'évaluation
- Proximal Humerus Fractures Epidemiology and TrendsDocument5 pagesProximal Humerus Fractures Epidemiology and TrendsHelena Sofia Fonseca Paiva De Sousa TelesPas encore d'évaluation
- Etamsylate DS Meppo2010 PDFDocument3 pagesEtamsylate DS Meppo2010 PDFAqmarlia PutriPas encore d'évaluation
- +++A Short Survey in Application of Ordinary Differential Equations On Cancer ResearchDocument5 pages+++A Short Survey in Application of Ordinary Differential Equations On Cancer ResearchEnes ÇakmakPas encore d'évaluation
- Secukinumab: First Global ApprovalDocument10 pagesSecukinumab: First Global ApprovalAri KurniawanPas encore d'évaluation
- DKA Handout1Document59 pagesDKA Handout1alePas encore d'évaluation
- Vitamin and Mineral Supplementation During PregnanDocument4 pagesVitamin and Mineral Supplementation During PregnanEvi RachmawatiPas encore d'évaluation
- The GINA 2019 Asthma Treatment Strategy For Adults and Adolescents 12... Download Scientific DiagramDocument1 pageThe GINA 2019 Asthma Treatment Strategy For Adults and Adolescents 12... Download Scientific DiagramFatih AryaPas encore d'évaluation
- TramadolDocument2 pagesTramadolJordanne EtisPas encore d'évaluation
- He2011 TMJ ANKYLOSIS CLASSIFICATIONDocument8 pagesHe2011 TMJ ANKYLOSIS CLASSIFICATIONPorcupine TreePas encore d'évaluation
- Ashiq Tutorials 2008Document23 pagesAshiq Tutorials 2008Sk ChaudhryPas encore d'évaluation
- Celiac DiseaseDocument35 pagesCeliac DiseaseRye HanaPas encore d'évaluation
- PMLS Lesson 5Document7 pagesPMLS Lesson 5Althea EspirituPas encore d'évaluation
- An Awareness Session On Blood Donation and Its ImportanceDocument40 pagesAn Awareness Session On Blood Donation and Its Importancekushi krishnaPas encore d'évaluation
- Bioengineering Transla Med - 2022 - Chopade - Alzheimer S and Parkinson S Disease Therapies in The ClinicDocument23 pagesBioengineering Transla Med - 2022 - Chopade - Alzheimer S and Parkinson S Disease Therapies in The ClinicurosPas encore d'évaluation