Académique Documents
Professionnel Documents
Culture Documents
685
Transféré par
EnfermagemFatern0 évaluation0% ont trouvé ce document utile (0 vote)
42 vues15 pagesCopyright
© © All Rights Reserved
Formats disponibles
PDF, TXT ou lisez en ligne sur Scribd
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentDroits d'auteur :
© All Rights Reserved
Formats disponibles
Téléchargez comme PDF, TXT ou lisez en ligne sur Scribd
0 évaluation0% ont trouvé ce document utile (0 vote)
42 vues15 pages685
Transféré par
EnfermagemFaternDroits d'auteur :
© All Rights Reserved
Formats disponibles
Téléchargez comme PDF, TXT ou lisez en ligne sur Scribd
Vous êtes sur la page 1sur 15
R E S U MO
Introduo: A Insuficincia Cardaca (IC) um
grave problema de Sade Pblica nos pases
desenvolvidos. Apesar dos enormes progressos
na abordagem da sndrome, o nmero de
internamentos por IC aguda e crnica agudizada
tem vindo a crescer, sendo j referida como o
primeiro motivo de internamento hospitalar
aps os 65 anos de idade, nos pases membros
da Sociedade Europeia de Cardiologia (SEC),
bem como nos Estados Unidos da Amrica do
Norte, na Austrlia e na Nova Zelndia. Os
estudos de populaes com IC aguda e crnica
agudizada so escassos e as primeiras
recomendaes para o diagnstico e teraputica
da Sociedade Europeia de Cardiologia s agora
foram publicadas.
Objectivos: Avaliar a prevalncia dos
internamentos por IC, na totalidade e por tipos
de disfuno cardaca, a co-morbilidade e os
factores desencadeantes da agudizao, no
Departamento de Medicina de um Hospital
Central em rea urbana, com actividade
assistencial e de ensino.
Populao e Mtodos: Estudo retrospectivo
observacional de doentes internados
consecutivamente a partir do Servio de
Urgncia Geral, entre Janeiro e Junho de 2001.
Procedeu-se reviso das notas de alta de todos
os internamentos, num total de 1038, e seleco
dos processos com diagnstico de IC data da
alta hospitalar ou de patologia do foro
cardiovascular precursora de IC. Foram
includos no estudo todos os doentes que
preenchiam os critrios para diagnstico de IC,
de acordo com as Recomendaes da SEC. Os
casos de IC identificados e includos foram
avaliados quanto s caractersticas
demogrficas, prevalncia global da sndrome e
ARTIGOS ORIGINAIS
Insuficincia Cardaca Aguda: Caractersticas
de uma Populao Hospitalar e Oportunidades
para a Melhoria dos Cuidados Prestados
[
2
]
PEDRO MORAES SARMENTO, CNDIDA FONSECA, FILIPA MARQUES, FTIMA CEIA, ANA ALEIXO,
Servio Universitrio de Medicina, Hospital de S. Francisco Xavier,
Faculdade de Cincias Mdicas, Universidade Nova de Lisboa
Lisboa, Portugal
A B S T R A C T
Acutely Decompensated Heart Failure:
Characteristics of Hospitalized Patients
and Opportunities to Improve their Care
Heart failure (HF) remains a major public
health problem in western countries, despite the
enormous progress in its diagnosis and
treatment. Acute and chronic decompensated
HF are leading medical causes of
hospitalization among people aged over 65
years in European countries, the USA, Australia
and New Zealand. However, there have been
few studies on acute and chronic
decompensated HF and the European Society of
Cardiology (ESC) guidelines on this subject
have only just been published.
Aim: To evaluate the overall prevalence of
hospitalization due to HF according to its
subtypes, comorbidities, and decompensating
factors, in the Medical Department of a central
teaching hospital in an urban area.
Methods: We performed a retrospective
observational study of patients admitted
consecutively to the Medical Department via
the emergency room between January and June
2001. Discharge casenotes on 1038 admissions
were reviewed. Those with a diagnosis of HF or
cardiovascular conditions associated with or
precursors of HF were analyzed. Cases with a
final diagnosis of HF according to the criteria of
the ESC guidelines were included in the study.
We evaluated the overall prevalence of HF and
subtypes of cardiac dysfunction, etiological risk
factors, patients demographic characteristics,
decompensating factors, comorbidity, mean
length of hospital stay, and in-hospital mortality
rate.
Recebido para publicao: Junho 2005 Aceite para publicao: Novembro 2005
Received for publication: June 2005 Accepted for publication: November 2005
Rev Port Cardiol 2006; 25 (1) : 13-27
ARTIGO 26-05-2006 15:26 Page 13
14
Rev Port Cardiol
Vol. 25 Janeiro 01/January 01
dos vrios tipos de disfuno cardaca, factores
etiolgicos/de risco, factores precipitantes da
agudizao, co-morbilidade, demora mdia do
internamento e mortalidade intra-hospitalar.
Resultados: Identificados 180 doentes com IC
(17,4%), com idade mdia de 74,614 anos, 87
do gnero masculino (48%) com idade mdia de
73,714,2 anos e 93 do gnero feminino (52%)
com idade mdia de 75,614 anos.
A IC por disfuno sistlica do VE (DSVE)
esteve presente em 42,2% dos casos, a IC com
funo sistlica preservada em 32,8% e a doena
valvular em 10,6%. A hipertenso arterial (HTA)
foi o principal factor etiolgico/predisponente
(62,2%), seguida da doena das artrias
coronrias (42,8%). Vinte e um vrgula seis por
cento dos doentes tinham diagnstico de diabetes
mellitus e 43,3%, fibrilhao auricular. Anemia
e doena pulmonar crnica obstructiva foram
registadas em cerca de um tero dos casos. No
que se refere a factores de agudizao da IC,
foram identificadas a infeco, sobretudo
respiratria, seguida da HTA no controlada e da
disritmia supraventricular com frequncia
ventricular rpida. entrada, estavam em classe
III da NYHA 42,2% e 44,8% em classe IV. A
demora mdia de internamento no Departamento
de Medicina neste perodo foi de 14,5 dias e a
dos doentes com IC de 13,8 dias; a mortalidade
intra-hospitalar por IC foi 7,7%. A IC foi a
primeira causa de internamento no
Departamento de Medicina no perodo estudado.
Concluses: Os dados confirmam a elevada
prevalncia de doentes com IC aguda ou
crnica agudizada em Departamentos de
Medicina. Os doentes so maioritariamente
idosos de ambos os sexos, com predomnio da
IC por DSVE, contrariamente ao recentemente
relatado para o ambulatrio em Portugal, onde
predomina a IC com funo sistlica preservada
e o sexo feminino. A maioria dos doentes estava
em classes III e IV da NYHA. A demora mdia
no foi superior dos restantes doentes e a
mortalidade intra-hospitalar foi baixa. A
elevada prevalncia da sndrome, o grupo
etrio, com mltipla co-morbilidade, enfatizam
a necessidade de uma abordagem complexa,
multidisciplinar, especializada, justificam a
criao de clnicas de IC e obrigam a um
esforo de consciencializao das entidades
para a sade nesta rea.
Results: We identified 180 patients with HF
(17.4%), mean age 74.614; 87 were male
(48%), aged 73.714.2, and 93 female (52%),
aged 75.614. Left ventricular systolic
dysfunction (LVSD) was present in 42.2% of
cases, preserved left ventricular systolic
function in 32.6%, and valvular heart disease in
10.6%. Hypertension and coronary artery
disease were the main etiological risk factors
(62.2% and 42.8% respectively). Atrial
fibrillation was recorded in 43.4% of the
patients, diabetes was diagnosed in 21.6%, and
anemia and chronic obstructive pulmonary
disease in about one third. Infection,
predominantly respiratory, was the main factor
triggering decompensation, followed by
uncontrolled hypertension and supraventricular
tachyarrhythmia. At admission, 42.2% of the
patients were in NYHA class III and 44.8% in
NYHA class IV. HF patients had a mean
hospital stay of 13.8 days, slightly shorter than
the mean overall stay of patients admitted to the
Medical Department in the same period (14.5
days). In-hospital mortality for HF patients was
7.7%, with HF being the first cause of
admission to the Medical Department, followed
by stroke (10.6%).
Conclusions: This study confirms the high
prevalence of acute or chronic decompensated
HF in patients hospitalized in the Medical
Department of a central teaching hospital in an
urban area. The patients were mainly elderly, of
both genders, with a slightly higher proportion
of HF due to LVSD. Most patients were in
NYHA classes III and IV. Mean hospital stay
was no longer than that of all patients admitted
in the same period. The in-hospital mortality
rate was low. The age-group affected and the
high prevalence of multiple comorbidities
emphasize the need to establish HF clinics with
multidisciplinary teams to manage these
patients, and health authorities must be made
aware of the burden of this syndrome.
Palavras-Chave
Insuficincia Cardaca Aguda; Internamento Hospitalar;
Co-Morbilidades
Key words
Acute Heart failure; Hospitalization; Heart Failure Clinics;
Co-morbidity
ARTIGO 26-05-2006 15:26 Page 14
INTRODUO
A
insuficincia cardaca (IC) uma situao
grave, com prevalncia crescente que,
apesar das muitas possibilidades de tratamento,
farmacolgico e no farmacolgico hoje
existentes, permanece uma condio
incapacitante, com mortalidade elevada,
necessitando frequentemente de internamento
hospitalar
(1-5)
. A IC responsvel por grande
consumo de meios assistenciais, onde o
internamento hospitalar representa mais de
75% dos gastos globais com a IC
(6-9)
. Em
Portugal, a prevalncia da insufi-cincia car-
daca crnica (ICC) nos adultos maio-
res de 25 anos de 4,36%, devendo atingir
mais de 260 000 pessoas
(10)
. A hipertenso
arterial (HTA) mantm-se como factor de
risco/etiolgico de maior prevalncia para IC,
seguido da doena coronria e da doena car-
daca valvu-lar
(10-12)
. A IC afecta sobretudo
indivduos com mais de 60 anos, sendo em
regra elevada a prevalncia da IC com funo
sistlica preserva-
da
(10, 12-14)
. Nestes escales etrios, a pluri-
patologia muito frequente, condicionando
particularidades de diagnstico e de tratamento,
pelo que o diagnstico diferencial da IC mais
complexo. Os falsos negativos so mais
frequentes
(15-19)
, a poli-medicao a regra e o
risco de efeitos adversos cresce
exponencialmente
(20-23)
. Existe evidncia
consistente de que a especializao no
tratamento da IC, com recurso a programas
integrados de tratamento e a clnicas de IC traz
benefcios ao tratamento destes doentes
(9, 24-28)
.
Para um correcto tratamento da sndrome
fundamental que se obtenha um diagnstico
preciso, sendo imprescindvel a caracterizao
anatmica e funcional da disfuno cardaca. O
internamento fornece uma boa oportunidade
para a caracterizao deste diagnstico
(8, 29, 30)
.
No entanto, em inqurito do Grupo de Estudo
de Insuficincia Cardaca da Sociedade
Portuguesa de Cardiologia, dirigido aos
Directores dos Servios de Cardiologia e de
Medicina Interna em Portugal, em 2000, foram
verificadas algumas carncias a nvel do
diagnstico e do tratamento aquando do
internamento, em ambos os tipos de Servios,
com um empenho claro e urgente na obteno
do parecer do Cardiologista e na realizao do
ecocardiograma, por parte dos Servios de
Medicina Interna, e na maior especializao de
INTRODUCTION
H
eart failure (HF) is a serious disease with
increasing prevalence; despite the many
pharmacological and non-pharmacological
treatment options now available, it is debilitating,
frequently requires hospitalization and has high
mortality
(1-5)
. It consumes a large proportion of
health resources, with hospitalization
representing over 75% of overall expenditure
on HF
(6-9)
. In Portugal, the prevalence of chronic
HF in adults aged over 25 is 4.36%, affecting
more than 260 000 people
(10)
. Hypertension
(HT) is the main etiological risk factor in HF,
followed by coronary artery disease and
valvular heart disease
(10-12)
. It affects mainly
individuals aged over 60, with a generally high
prevalence of HF with preserved systolic
function
(10, 12-14)
. A high level of comorbidity is
common in this age-group, which has particular
relevance for diagnosis and treatment and
makes differential diagnosis of HF more
difficult. False negatives are common
(15-19)
,
polypharmacy is the general rule and the risk of
adverse effects increases exponentially
(20-23)
.
There is solid evidence that specialist HF
treatment, with integrated management
programs and HF clinics, is beneficial to these
patients
(9, 24-28)
. In order to treat this syndrome
correctly, it is essential to obtain an accurate
diagnosis, for which anatomical and functional
characterization of cardiac dysfunction are
required. Hospitalization provides a good
opportunity for such characterization
(8, 29, 30)
. How-
ever, a survey by the Portuguese Society
of Cardiologys Heart Failure Working Group,
addressed to the heads of cardiology and
internal medicine departments in Portugal in
2000, showed certain deficiencies in diagnosis
and treatment during hospitalization in both
types of department. In the case of internal
medicine departments, there was a clear and
urgent need to obtain a cardiologists opinion
and perform an echocardiogram, and a need for
more specialist training for doctors and nurses
and the establishment of HF clinics in
cardiology departments
(31, 32)
. It is well known
that HF treatment, even in developed countries,
is far from ideal. With regard to HF with left
ventricular systolic dysfunction (LVSD), for
which there are explicit guidelines, recent stud-
ies have shown that major efforts need to be
made in primary care in Europe to improve the
use of drugs that reduce mortality, morbidity
and hospitalization
(11, 33)
; the same was observed
PEDRO MORAES SARMENTO, et al
Rev Port Cardiol 2006; 25: 13-27
ARTIGO 26-05-2006 15:26 Page 15
mdicos e enfermeiras, com criao de clnicas
de IC, por parte dos servios de cardiologia
(31,32)
.
conhecido que o tratamento da IC, mesmo
nos pases evoludos, est longe de ser o mais
correcto. No que se refere IC por disfuno
sistlica ventricular esquerda (DSVE), para a
qual existem recomendaes definidas, estudos
recentes mostraram que, na Europa, no
ambulatrio, tem de haver um importante
trabalho de melhoria da utilizao dos frmacos
que permitem diminuir a mortalidade e reduzir
a morbilidade e a hospitalizao
(11, 33)
; o mesmo
foi observado em Portugal, no estudo EPICA
(10,
34)
.
So escassos os trabalhos referentes ao
internamento de doentes com IC aguda ou
crnica agudizada em Portugal. Assim, numa
fase de implementao de uma Unidade
Funcional de IC e como base para o
conhecimento das necessidades assistenciais,
decidimos avaliar as caractersticas
epidemiolgicas dos doentes internados por IC
no Departamento de Medicina do Hospital de S.
Francisco Xavier, a prevalncia global da
sndrome e dos vrios tipos de disfuno car-
daca no internamento, bem como dos factores
etiolgicos, co-morbilidade e de agudizao.
METODOLOGIA
Estudo retrospectivo observacional de doen-
tes internados consecutivamente entre Janeiro e
Junho de 2001, no Servio de Medicina do
Hospital de S. Francisco Xavier, hospital com
actividade assistencial e de ensino, em rea
urbana, com urgncia geral aberta e
internamento pela urgncia, servindo uma
populao de aproximadamente 400 000
habitantes. O Servio de Medicina funciona
como Departamento, sem internamento electivo
em Cardiologia, dispondo de Laboratrios
prprios com acesso directo s tcnicas
complementares de diagnstico e de
teraputica, de Cardiologia e de outras
Especialidades, assegurando actividade
assistencial em equipa multidisciplinar com a
Medicina Interna.
Foram revistas as notas de alta, com
seleco e reviso subsequente de todos os
registos de internamento no Servio de
Medicina, com diagnstico de sada de: IC,
ICC, ou de doena cardiovascular precursora de
IC (estadios A e B das recomendaes da
ACC/AHA
(30)
: doena das artrias coronrias 16
in Portugal in the EPICA study
(10, 34)
.
There are few studies on hospitalization of
patients with acute or chronic decompensated
HF in Portugal. As part of the process of
establishing an HF unit and determining the
resources required, we decided to evaluate the
epidemiological characteristics of patients
admitted for HF to the Medical Department of
S. Francisco Xavier Hospital, the overall
prevalence of the syndrome and the various
subtypes of cardiac dysfunction at admission,
as well as etiological factors, comorbidities and
decompensating factors.
METHODS
We performed a retrospective observational
study of patients admitted consecutively be-
tween January and June 2001 to the Medical
Department of S. Francisco Xavier Hospital,
which is a central teaching hospital in an urban
area, with an open general emergency room and
admission via the emergency room, serving a
population of approximately 400 000. The Med-
ical Department has no elective admission in
cardiology, but has its own laboratories with
direct access to diagnostic and therapeutic
techniques in cardiology and other
specializations, and a multidisciplinary team
providing treatment in collaboration with the
Internal Medicine Department.
The discharge casenotes were reviewed,
with selection and subsequent analysis of all
the patients admitted to the Medical
Department with a discharge diagnosis of HF or
c a r d i o -
vascular conditions associated with or
precursors of HF (stages A and B of the
ACC/AHA guidelines
(30)
): coronary artery
disease in its various clinical forms, HT,
cardiomyopathy, valvular heart disease,
congenital cardiovascular disease, pericardial
disease, cor pulmonale and atrial fibrillation
(AF). Epidemiological, electrocardiographic,
radiographic and echocardiographic data were
recorded, together with findings from other
techniques used to characterize cardiac
dysfunction (digital coronary angiography and
ventriculography and radionuclide
angiography), as well as information on clinical
pathology relevant to the diagnosis of HF and
its etiology, risk and triggering factors, and
comorbidities. In accordance with the European
Society of Cardiology (ESC) guidelines
(29)
, the
Rev Port Cardiol
Vol. 25 Janeiro 01/January 01
ARTIGO 26-05-2006 15:26 Page 16
nas suas vrias formas clnicas, HTA,
miocardiopatia, doena cardaca valvular,
doena cardiovascular congnita, doen-
a do pericrdio, cor pulmonale e fibrilhao
auricular (FA). Foram registados os dados
epidemiolgicos, electrocardiogrficos,
radiolgicos, ecocardiogrficos e de outros
mtodos de caracterizao da disfuno car-
daca (coronario-ventriculografia digital e
angiografia de radionucldeos), bem como de
patologia clnica, relevantes para o diagnstico
de IC e da sua etiologia, dos factores
predisponentes e precipitantes e das
comorbilidades. Foram considerados critrios
para o diagnstico de IC, de acordo com as
recomendaes da Sociedade Europeia de
Cardiologia (SEC)
(29)
, a presena de clnica de
IC (e/ou de resposta clnica favorvel a
teraputica dirigida) com evidncia objectiva
de disfuno cardaca em repouso, obtida por
mtodo de imagem (ecocardiografia
transtorcica bidimensional e Doppler ou
ventriculografia por angiografia digital ou
isotpica), em exames efectuados durante o
internamento. Foi tambm considerada a
caracterizao de disfuno cardaca, quando
efectuada nos 6 meses anteriores ao
internamento e quando reveladora de DSVE. Os
casos de IC foram classificados em: IC por
DSVE, IC com funo sistlica do VE
preservada, IC por doena cardaca valvular, IC
direita, IC multifactorial, IC por cardiopatia
congnita e FA isolada (Quadro I)
(10, 35-40)
. O
diagnstico de HTA foi admitido na presena
de diagnstico prvio ou de medicao com
frmacos anti-hipertensivos e/ou de presso
arterial superior a 140/90 mm Hg ou 130/80
mm Hg, se coexistncia de diabetes mellitus. O
diagnstico de doena das artrias coronrias
foi considerado na presena de histria prvia
de enfarte do miocrdio, de coronariografia
positiva e/ou de isquemia documentada em
prova de esforo ou cintigrafia do miocrdio; a
doena cardaca valvular quando comprovada
por ecocardiografia bidimensional e Doppler
(42)
.
Foi considerado o diagnstico de anemia para
valores de hemoglobina 12 g/dl, e o de
insuficincia renal quando a creatininemia foi
2,5 mg/dl. O diagnstico de doena pulmonar
obstrutiva crnica (DPOC) exigiu diagnstico
prvio, com presena de histria de doena
respiratria crnica e de insuficincia
respiratria. Considermos diagnstico de
diabetes mellitus a presena de diagnstico
criteria used for a diagnosis of HF were a
clinical setting of HF (and/or a positive
response to directed therapy), with objective
evidence of cardiac dysfunction at rest by imag-
ing techniques (two-dimensional transthoracic
and Doppler echocardiography or
ventriculography by digital or radionuclide
angiography) performed during hospitalization.
Characterization of cardiac dysfunction was
also included if performed in the six months
prior to admission and revealed LVSD. HF
cases were classified as: due to LVSD, with
preserved LV systolic function, due to valvular
heart disease, right HF, multifactorial HF, due
to congenital heart disease, and isolated AF
(Table I)
(10, 35-40)
. HT was considered present if
there was a previous diagnosis, medication with
antihypertensive drugs and/or blood pressure
above 140/90 mmHg or 130/80 mmHg in the
presence of diabetes. Coronary artery disease
was diagnosed on the basis of previous history
of myocardial infarction, positive coronary
angiography and/or documented ischemia on
exercise testing or myocardial scintigraphy, or
valvular heart disease when confirmed by two-
dimensional and Doppler echocardiography
(42)
.
A diagnosis of anemia was based on hemo-
globin values of 12 g/dl, and of renal failure if
creatininemia was 2.5 mg/dl. Chronic
obstructive pulmonary disease (COPD) was
considered present if there was a previous
diagnosis and a history of chronic respiratory
disease or failure, and diabetes in the presence
of a previous diagnosis with directed therapy, or
de novo, in accordance with the recommended
criteria
(41)
. Any triggering factors recorded in
the clinical records by the attending physicians
were also recorded. Patients hospitalized
exclusively in intensive care units were
excluded from the study.
POPULATION
Out of a total of 1038 admissions in the
period under study, 234 cases of possible HF
were identified, of which 54 were subsequently
excluded as they did not meet the predefined
diagnostic criteria.
RESULTS
One hundred and eighty patients (17.4%)
had HF according to the criteria. Mean age was
74.614 years; 87 were male (48%), mean age
PEDRO MORAES SARMENTO, et al
Rev Port Cardiol 2006; 25: 13-27
ARTIGO 26-05-2006 15:26 Page 17
prvio, com tratamento dirigido, ou de novo, de
acordo com os critrios recomendados
(41)
. Foram
registados os factores precipitantes de acordo
com a informao constante nos processos pelos
respectivos mdicos assistentes. Os doentes
internados exclusivamente nas Unidades de
Cuidados Intensivos Coronria (UNICARD) e
Mdicos (UCIM), foram excludos deste estudo.
POPULAO
Num total de 1038 internamentos
contabilizados no perodo estudado, foram
identificados 234 casos de IC possvel, dos
quais 54 foram excludos, por no preencherem
os critrios de diagnstico pr-definidos.
18
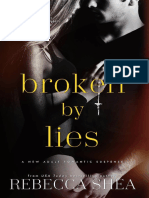
73.714.2, and 93 female (52%), mean age
75.614; 36% of the patients were aged over
80. HT was the principal etiological risk factor
for HF (62.2%), followed by coronary artery
disease (42.8%); diabetes was present in
21.6%. Almost half the patients were in AF
(43.3%). Anemia was recorded in 31.7% of
cases, COPD in 27.8%, and chronic renal
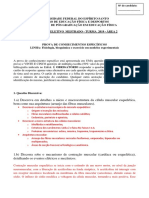
failure in 8.2% (Fig. 1). Infection,
predominantly respiratory, was the main factor
triggering decompensation (Fig. 2);
supraventricular tachy-
arrhythmia with rapid ventricular rate and
uncontrolled HT were recorded in 25% and
17.2% of patients respectively. Pulmonary
Rev Port Cardiol
Vol. 25 Janeiro 01/January 01
Quadro I
Sub-tipos de IC, definidos de acordo com critrios ecocardiogrficos, por angiografia digital
ou por angiografia de radionucldeos
(12, 36-39)
. Para caracterizao do subtipo foi seguida
a ordem descrita no Quadro (adaptado de Ceia e cols,
(10)
)
Insuficincia cardaca sub-tipo Definio/Critrios ecocardiogrficos
IC devida a doena cardaca valvular Doena valvular moderada ou grave
IC devida a doena do pericrdio Anomalia ou derrame pericrdico moderado ou grave
IC direita Dilatao isolada do VD, ou associada a dilatao da AD
IC por disfuno sistlica do VE Fraco de ejeco do VE <40%, ou Fraco de encurtamento do VE <28%,
ou alterao grave da cintica segmentar associada a dilatao do VE
IC com funo sistlica preservada Na ausncia de qualquer das anteriores anomalias e na presena de dilatao
da AE*, ou de aumento do ndice de massa do VE, ou de aumento da espessura
do septo inter-ventricular ou da parede posterior do VE associada a dilatao
do VE**
IC multifactorial Quando se registaram vrias anomalias, no sendo possvel identificar
a responsvel primria
IC por fibrilhao auricular isolada Na presena de quadro clnico de IC
(30)
, na ausncia de quaisquer outras
anomalias, com excepo de fibrilhao auricular
IC: Insuficincia cardaca; VD: ventrculo direito; AD: aurcula direita; AE: aurcula esquerda. * Dimenso da AE superior ao percentil 95 do
valor previsto em funo da idade e superfcie corporal. ** ndice de massa ventricular esquerda >134 g/m
2
no homem e >110 g/m
2
na mulher;
dimenses da parede posterior ou septo inter-ventricular superiores ao percentil 95 do valor previsto em funo da idade e superfcie corporal,
quando no existiram dados para calcular o ndice de massa do VE; Os valores previsveis para o sexo, idade e superfcie corporal foram
calculados pelas equaes de Henry
(39)
.
Table I
HF subtypes, defined according to echocardiographic and digital or radionuclide angiographic criteria
(12, 36-
39)
. To characterize the subtype, the order in the table was followed (adapted from Ceia et al.
(10)
)
Heart failure subtype Definition/Echocardiographic criteria
HF due to valvular heart disease Moderate or servere valve disease
HF due to pericardial disease Moderate or severe pericardial abnormality or effusion
Right HF RV dilatation, isolated or associated with RA dilatation
HF due to LVSD LV ejection fraction <40%, or LV fractional shortening <28%, or severe
segmental kinetic abnormality associated with LV dilatation
With PSF Left atrial dilatation*, or increased LV mass index, or increased interventricular
septum or LV posterior wall tickness, associated with LV dilatation**, in the
absence of any of the previously mentioned abnormalities:
Multifactorial HF Cases with various abnormalities, in which it is impossible to identify the primary
cause
HF due to isolated AF Cases with a clinical setting of HF
(30)
, but no other abnormalities apart from atrial
fibrillation
HF: heart failure; RC: right ventricle; LV: left ventricle; RA: right atrium; LVSD: left ventricular systolic dysfunction; PSF: preserved systolic
function; AF: atrial fribrillation; LA: left atrium. * LA size above percentile 95 of the predicted value for age and body surface area; ** Left
ventricular mass index >134 g/m
2
in men and >110 g/m
2
in woman; dimensions of posterior wall and ventricular septum above percentile 95 of
the predicted value for age and body surface area if no data were available to calculate LV mass index. The predicted values for gender, age and
body surface area were calculated using henrys equations
(39)
.
ARTIGO 26-05-2006 15:26 Page 18
RESULTADOS
180 doentes (17,4%) tinham IC de acordo
com os critrios definidos. A idade mdia foi de
74,614 anos; 87 eram do gnero masculino
(48%) com idade mdia de 73,714,2 anos e 93
do feminino (52%) com idade mdia de
75,614 anos; 36% dos doentes tinham idade
superior a 80 anos. A HTA foi o principal factor
etiolgico/predisponente para IC (62,2%),
seguida da doena das artrias coronrias, em
42,8% dos doentes; a diabetes mellitus estava
presente em 21,6%. Quase metade dos doentes
estava em FA (43,3%). Foi registada anemia em
31,7% dos casos, DPOC em 27,8% e insuficin-
cia renal crnica em 8,2% (Fig. 1). No que
se refere a factores desencadeantes de
descompensao da IC (Fig. 2), a infeco foi o
de maior prevalncia, sobretudo a infeco
respiratria; disritmia supraventricular com
frequncia ventricular rpida e HTA no
controlada foram registadas em 25% e 17,2%
dos doentes, respectivamente. Em 2,2% dos
casos foi diagnosticado tromboembolismo
pulmonar. A m adeso teraputica foi
identificada como factor de descompensao
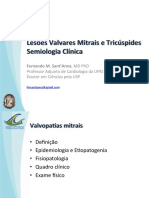
em 5% dos internamentos. No que se refere aos
tipos de IC (Fig. 3), a IC por DSVE estava
presente em 42,2% dos casos, a IC com funo
sistlica preservada em 32,8% e a doena
valvular em 10,6%; 3,9% tinham FA isolada.
Quanto gravidade do compromisso funcional
entrada, de acordo com a classificao da
thromboembolism was diagnosed in 2.2% of
cases. Poor compliance with therapy was
identified as a decompensating factor in 5% of
hospitalizations. With regard to type of heart
failure (Fig. 3), HF due to LVSD was found in
42.2% of cases, and HF with preserved systolic
function in 32.8%, and valve disease in 10.6%;
3.9% had isolated AF. Regarding severity of
functional impairment at admission, 11% were
in NYHA class II, 42.2% in class III and
44.8% in class IV; no patient was in class I.
There was no reference to NYHA class in 2% of
cases.
Mean hospital stay was 13.8 days, the mean
for all patients admitted to the Medical
Department in the same period being 14.5 days.
In-hospital mortality for HF patients was 7.7%,
overall mortality in the Medical Department
being 9.3%. HF was the first cause of
admission to the Medical Department during
the period under study (17.4%), followed by
stroke (10.6%).
DISCUSSION
Heart failure is a common cause of
hospitalization in medical departments in
Portugal, as in many other European countries
(3,
5, 33, 42-45)
. The EuroHeart Survey on Heart Failure,
which stud-
ied patients admitted with HF to 115 hospitals
in 24 member countries of the ESC, confirmed
PEDRO MORAES SARMENTO, et al
Rev Port Cardiol 2006; 25: 13-27
Fig. 1 Factores etiolgicos/de
risco e co-morbilidades em
doentes internados por IC em
Departamento de Medicina.
HTA: hipertenso arterial;
DAC: doena das artrias
coronrias; FA: fibrilhao
auricular; DPOC: doena
pulmonar obstructiva crnica;
IRC: insuficincia renal
crnica.
Fig. 1 Etiological risk factors
and comorbidities in patients
hospitalized for HF in the
Medical Department. HT:
hypertension; CAD: coronary
artery disease; AF: atrial
fibrillation; COPD: chronic
obstructive pulmonary disease;
CRF: chronic renal failure.
ARTIGO 26-05-2006 15:26 Page 19
NYHA, 11% estavam em classe II, 42,2% em
classe III e 44,8% em classe IV; no se
observou nenhum doente em classe I. A classe
da NYHA no estava mencionada em 2% dos
casos.
A demora mdia do internamento foi de 13,8
dias, sendo a demora mdia da totalidade dos
doentes internados no Departamento de
Medicina, no mesmo perodo, 14,5 dias. A
mortalidade intra-hospitalar por IC foi 7,7%,
tendo sido a mortalidade global no
Departamento de Medicina, 9,3%. A IC foi a
primeira causa de internamento no
Departamento de Medicina no perodo estudado
(17,4%), seguida do acidente vascular cerebral
(10,6%).
DISCUSSO
A IC causa frequente de internamento
hospitalar em servios de medicina, entre ns
como em muitos outros Pases na Europa
(3, 5, 33, 42-
4 5 )
.
O EuroHeart Survey on Heart Failure, que
estudou doentes internados com IC em 115
hospitais nos 24 pases membros da SEC,
comprovou que a IC foi a principal causa do
internamento nesses hospitais (40%), sendo
metade dos doentes internados em servios de
medicina (50%)
(33)
. Naquele estudo verificou-se
que a idade mdia dos doentes internados por
IC variou entre 63 e 75 anos, havendo um claro
20
that HF was the leading cause of hospitalization
(40%), with half the patients admitted to
medical departments (50%)
(33)
. The study found
that the mean age of patients admitted for HF
ranged between 63 and 75 years, with a clear
predominance of women aged over 75 in most
countries, particularly the United Kingdom,
Scandinavia, France and Switzerland
(33)
. Similar
findings were reported in Italy by the
TEMISTOCLE study investigators, relating to
HF patients admitted to 250 internal medicine
hospital units (62.9% of the total number of pa-
tients studied): 52.1% were female (vs. 38.4%
in cardiology), mean age was 7710 years (vs.
7012 in cardiology), and mean hospital stay
was 11.5 days
(46)
. In our study, the patients
admitted for HF were also predominantly
elderly and with severe functional impairment
(over 80% in NYHA classes III and IV), around
half were women, and a third had HF with
preserved systolic function. Hypertension and
coronary artery disease were the most common
etiological factors, as in all industrialized
countries
(13, 33, 47, 48)
. In most European countries,
the prevalence
of coronary artery disease as the main
etiological factor in patients hospitalized for HF
is higher than that found in our study (42.8%),
ranging from 37% in Spain to 84% in
Lithuania, with a mean of 68%
(33)
. Acute
coronary syndromes are a common cause of
acute or chronic decompensated HF requiring
Rev Port Cardiol
Vol. 25 Janeiro 01/January 01
Fig. 2 Doentes internados por
IC aguda ou crnica agudizada
em Departamento de Medicina:
factores desencadeantes da
agudizao. Infec. Resp.:
infeco respiratria; HTA:
hipertenso arterial; SCA:
sndromes coronrias agudas;
SV: supraventricular; TEP:
tromboembolismo pulmonar.
Fig. 2 Patients hospitalized for
acute or chronic decompensated
HF in the Medical Department:
decompensating factors.
Resp. Inf.: respiratory infection;
Ucont: uncontrolled; HT:
hypertension; ACS: acute
coronary syndrome; SV:
supraventricular; PTE:
pulmonary thromboembolism.
ARTIGO 26-05-2006 15:26 Page 20
predomnio de mulheres com mais de 75 anos
na maioria dos pases, especialmente no Reino
Unido, Escandinvia, Frana e Suia
(33)
; dados
semelhantes foram encontrados em Itlia pelos
investigadores do estudo TEMISTOCLE, no que
se refere aos doentes com IC internados em 250
servios de medicina interna (62,9% da
totalidade dos doentes estudados): 52,1% eram
mulheres (vs 38,4%, na Cardiologia), a idade
mdia foi de 7710 anos (vs 7012 anos, na
Cardiologia), e a demora mdia do internamento
foi 11,5 dias
(46)
. Tambm no nosso estudo os
doentes hospitalizados por IC foram
predominantemente idosos com grave
compromisso funcional (mais de 80% nas
classes III e IV da NYHA), sendo cerca de
metade mulheres e um tero, doentes com IC e
funo sistlica preservada. Os factores
etiolgicos mais frequentes da IC foram a HTA
e a doena coronria, tal como acontece nos
pases industrializados
(13, 33, 47, 48)
. Na Europa, a
prevalncia da doena das artrias coronrias
como factor etiolgico de IC em doentes
internados , na maioria dos pases, superior
encontrada no nosso estudo (42,8%), variando
entre 37% em Espanha e 84% na Litunia,
sendo, em mdia, de 68%
(33)
. As sndromes
coronrias agudas so causa frequente de IC
aguda ou crnica descompensada, necessitando
de internamento
(33)
; no nosso estudo, foram
registadas em 13,3% dos doentes.
A percentagem mdia de doentes internados
hospitalization
(33)
, as was the case in 13.3% of
the patients in our study.
The mean percentage of patients with HT
hospitalized for HF in Europe was 53%,
ranging between 22 and 70%, with a tendency
for higher rates in Mediterranean countries and
central Europe
(33)
, but lower than that observed
in the present study. The high prevalence of HT
in Portugal and low rate of control (estimated to
be only 11%)
(49)
may have been factors trig-
gering decompensation and leading to hospitaliza-
tion in a fifth of our patients. The present study
confirms that HT is the main etiological risk
factor for all types of HF due to ventricular
failure in Portugal, highlighting the importance
of implementing vigorous measures for its
treatment and prevention.
Almost half the patients were in AF, a find-
ing also reported by the EuroHeart survey and
other authors analyzing hospitalization of
elderly patients with HF
(33, 45)
. The presence of a
rapid ventricular rate as a factor in
decompensation, observed in a quarter of cases,
emphasizes the need for effective heart rate
control and oral anticoagulation
(29, 50, 51)
. The
incidence of pulmonary thromboembolism,
although similar in our study to the average
reported by the
EuroHeart survey (3%)
(33)
, is probably underesti-
mated in both cases, since postmortem studies
show a much higher incidence than in vivo
studies, of up to 70%
(45, 52, 53)
. There is an urgent
PEDRO MORAES SARMENTO, et al
Rev Port Cardiol 2006; 25: 13-27
Fig. 3 IC no internamento em
Departamento de Medicina:
prevalncia dos diferentes sub-
grupos etiopatognicos e
fisiopatolgicos. DSVE:
disfuno sistlica do VE; FSP:
funo sistlica preservada; IC
dta: insuficincia cardaca
direita; FA: fibrilhao
auricular; DC: doen-a cardaca;
Cong: congnita mul-
tifactorial.
Fig. 3 HF patients admitted to
the Medical Department:
prevalence of the different
etiopathogenic and
pathophysiologic subgroups.
LVSD: left ventricular systolic
dysfunction; PSF: Preserved
systolic function; RHF: right
heart failure; AF: atrial
fibrillation; Multifact HF:
ARTIGO 26-05-2006 15:26 Page 21
por IC com HTA foi, na Europa, de 53%, com
variao entre 22 e 70%, tendencialmente mais
elevada nos Pases da Bacia Mediterrnica e da
Europa Central
(33)
, mas inferior por ns
observada. A elevada prevalncia de HTA em
Portugal e o seu insuficiente controlo
teraputico, estimado em apenas 11% dos
doentes
(49)
, podem ter sido factores
desencadeantes da agudizao e do
internamento, em cerca de 1/5 dos nossos
doentes. O presente estudo veio confirmar que
a HTA o principal factor etiolgico/de risco
para todos os tipos de IC por falncia ventricu-
lar em Portugal, atestando da importncia da
instituio de medidas vigorosas no seu
tratamento e preveno.
Quase metade dos doentes estava em FA, o
que tambm referido pelo EuroHeart Survey e
por outros autores que analisaram o
internamento de idosos com IC
(33, 45)
. A
ocorrncia de frequncia ventricular rpida
como factor de agudizao, observada em
1
/4 dos
casos, apela necessidade da instituio de
teraputica adequada para o controlo da
frequncia cardaca e da hipocoagulao oral
(29,
50, 51)
. Neste contexto, a incidncia de
tromboembolismo pulmonar, ainda que idntica
mdia referida pelo EuroHeart Survey 3%
(33)
, dever estar sub-estimada em ambos os
estudos. Nos estudos post-mortem, esta
incidncia, muito mais elevada
do que a dos estudos in vivo, pode atingir os
70%
(45, 52, 53)
; urgente promover a educao dos
clnicos para este diagnstico e para a
instituio de medidas de preveno e de
tratamento adequadas.
A prevalncia do diagnstico de infeco em
doentes com IC hospitalizados, na Europa,
variou muito, sendo todavia frequentemente
elevada, sobretudo na Sucia, Irlanda e em
Espanha
(33)
. semelhana do referido na
Europa, tambm foi muito elevada entre ns,
particularmente a da infeco respiratria,
alertando para a necessidade da instituio de
medidas de preveno adequadas, nomeada-
mente a vacinao dos doentes em risco.
Admitimos que exista, no nosso estudo, um
enviesamento importante na avaliao da m
adeso teraputica como factor desencadeante
da agudizao, por se tratar de estudo
retrospectivo. No entanto, as percentagens de
adeso teraputica, medicamentosa e no-
medicamentosa, variam muito de estudo para 22
need to promote greater awareness of this entity
among clinicians and to implement effective
measures for its treatment and prevention.
The prevalence of a diagnosis of infection in
hospitalized HF patients in Europe varies
greatly, but is often high, particularly in Sweden,
Ireland and Spain
(33)
. It was also high in our
study, especially respiratory infection, which
underlines the need for appropriate prevention
measures, particularly vaccination of high-risk
patients.
We acknowledge that, since our study was
retrospective, this may have biased our
assessment of non-compliance with therapy as a
decompensating factor. However, the
percentage reported for compliance with
medication and other therapeutic measures
varies greatly between studies, ranging from 21
to 64%
(54)
. Educating patients and their families
on the importance of strict compliance with the
prescribed therapy should be a priority for staff
involved in treating patients with HF
(21, 24, 28)
.
Diabetes has long been known to be a risk
factor and an indicator of worse prognosis in
HF patients
(19, 55-57)
. Metabolic control is
essential to improve prognosis and reduce
hospital stays and rehospitalizations
(18, 57)
.
Around a fifth of the HF patients admitted to
our Department were diagnosed with diabetes, a
similar figure to that reported elsewhere
(33)
,
which means a multidisciplinary approach is
required.
The prevalence of anemia in HF patients
varies from study to study, largely because the
hemoglobin levels used for its diagnosis range
between 11 and 13 g/dl, but also because
prevalence varies according to NYHA
functional class. It is commonly found in over a
quarter of cases, as in our study
(19, 45, 58, 59)
. It is
often of multifactorial etiology and an
aggravating factor in morbidity and mortality
(58-
60)
. The frequent coexistence of anemia, HF and
renal failure constitutes the cardiorenal anemia
syndrome, which has a worse prognosis
(61)
.
Recent studies, with promising results, suggest
that parenteral administration of erythropoietin
and iron
(62)
to maintain hemoglobin levels above
12 g/dl can influence morbidity in this
syndrome, by improving functional capacity
and renal insufficiency. The effect of this ther-
apy on mortality has yet to be published.
The diagnostic criterion for renal failure that
we used (creatininemia >2.5 mg/dl), which
identifies only advanced renal failure, led to a
Rev Port Cardiol
Vol. 25 Janeiro 01/January 01
ARTIGO 26-05-2006 15:26 Page 22
estudo, entre 21 e 64%
(54)
. A educao do
doente e familiares para o tratamento e o
cumprimento rigoroso da prescrio deve
merecer particular ateno por parte dos
profissionais empenhados no tratamento dos
doentes com IC
(21, 24, 28)
.
A diabetes mellitus reconhecida desde h
muito como factor etiolgico e de pior
prognstico nos doentes com IC
(19, 55-57)
. O
controlo metablico fundamental para
melhorar o prognstico, reduzir o tempo de
hospitalizao e a necessidade de re-
internamento
(18, 57)
. semelhana do que tem
sido referido
(33)
, cerca de um quinto dos doentes
com IC internados no nosso servio tinham
diagnstico de diabetes mellitus, exigindo a
multidisciplinaridade das equipas assistenciais.
A prevalncia de anemia nos doentes com
IC varia de estudo para estudo, em grande parte
porque os valores de concentrao srica da
hemoglobina utilizados para o seu diagnstico
variam entre 11 e 13 g/dl, e porque a
prevalncia da anemia varia consoante a classe
funcional da NYHA. frequentemente
observada em mais de um quarto dos casos,
como sucedeu no nosso estudo
(19, 45, 58, 59)
.
Frequentemente tem etiologia plurifactorial e
constitui factor de agravamento da morbi-
mortalidade
(58-60)
. Frequente, a co-existncia de
anemia, IC e insuficincia renal, constitui uma
entidade designada como sndrome da anemia
cardio-renal, com prognstico agravado
(61)
.
Estudos recentes com resultados promissores,
sugerem que a administrao de eritropoietina
e ferro, por via parentrica
(62)
, de forma a
manter nveis de hemoglobina superiores a 12
g/dl, possa influenciar a morbilidade desta
sndrome, melhorando a capacidade funcional e
a insuficincia renal. Aguardam-se os
resultados na modificao da mortalidade.
O critrio de diagnstico de insuficincia
renal por ns utilizado (creatininemia >2,5
mg/dl), identificando apenas as situaes de
insuficincia renal avanada, fez com que a
prevalncia da insuficincia renal crnica fosse
inferior referida por outros autores. das co-
morbilidades com impacto mais negativo no
prognstico da IC, quanto ao tempo e
qualidade de vida
(48, 61, 63, 64)
. Exige medidas de
preveno adequadas e unidades
especializadas, no manejo da volemia, da
presso arterial, dos inibidores da enzima de
converso da angiotensina, dos antagonistas dos
lower prevalence of chronic renal failure than
that reported by other authors. It has one of the
greatest negative impacts of all comorbidities
on prognosis in HF, in terms of both survival
and quality of life
(48, 61, 63, 64)
. Effective preventive
measures and specialized units are therefore
required to manage volemia, blood pressure,
and therapy with angiotensin-converting
enzyme inhibitors and AT1 angiotensin II and
spironolactone receptor antagonists.
COPD is present in 20 to 30% of cases of
HF; it leads to worse prognosis in terms of
morbidity and mortality, makes differential
diagnosis more difficult, and requires
s p e c i a l i z e d
treatment
(19, 65)
. A diagnosis of COPD in patients
with LVSD can also influence the decision to
prescribe beta-blockers for fear of aggravating
bronchial hyperreactivity. However, it is
generally agreed that using these drugs does not
worsen respiratory failure in stabilized patients
without bronchial hyperreactivity who are past
the acute phase of respiratory disease
(13, 66)
.
We found that the prevalence of HF with
LVSD was almost the same as that with
preserv-ed systolic function, as is commonly
reported in similar populations of unselected
elderly patients with HT, coronary artery disease
and AF
(42, 67, 68)
. There is an urgent need for more
precise diagnostic criteria for this entity, as
well as for
treatment guidelines. It should be noted that in
our study a large number of patients had other
types of HF, mainly valvular heart disease, as
also found in the EuroHeart survey
(33)
; other
types of HF were less common, particularly
isolated right HF and multifactorial HF.
Mean hospital stay was within the range
reported for HF in Europe by Stewart et al. (8
days for men and 10 for women) and by Brown
and Cleland (11.3 days, with considerable
variability depending on concomitant disease);
Wright et al., in New Zealand, reported 6 days
(45)
. In the United States, the ADHERE study
showed a mean hospital stay of 4.5 days, which
is related largely to the existence of continuing
care facilities to which these patients are
transferred following hospital discharge; how-
ever, a high rate of rehospitalizations was also
recorded
(69)
. It should be noted that in the
EuroHeart survey, mean hospital stay ranged
between 7 and 19 days, and was longer than 10
days in 59% of the participating countries
(33)
.
Many factors influence duration of hospital
PEDRO MORAES SARMENTO, et al
Rev Port Cardiol 2006; 25: 13-27
ARTIGO 26-05-2006 15:26 Page 23
receptores AT1 da angiotensina II e da
espironolactona.
A DPOC coexiste em cerca de 20 a 30% dos
casos de IC e constitui tambm factor de mau
prognstico quanto morbi-mortalidade, coloca
problemas de diagnstico diferencial e exige
abordagem especializada
(19, 65)
. O diagnstico de
DPOC nos doentes com DSVE pode ainda
condicionar os clnicos na prescrio de
bloqueadores beta-adrenrgicos, por receio de
agravamento da bronco-reactividade. No
entanto, consensual que a utilizao destes
frmacos no agrava a insuficincia respiratria
nos doentes estabilizados, sem bronco-
reactividade e fora da fase aguda da doena
respiratria
(13, 66)
.
Verificmos que a prevalncia de IC por
DSVE foi quase igual da IC com funo
sistlica preservada, como frequentemente
referido em populaes semelhantes, de doen-
tes no seleccionados, idosos e muito idosos,
com HTA, doena coronria e FA
(42, 67, 68)
. So
urgentes a utilizao de critrios de diagnstico
mais precisos para esta entidade e a definio
de recomendaes de teraputica. De salientar
que, no nossos estudo, um nmero elevado de
doentes tinha IC de outros tipos, sobretudo
doena cardaca valvular, semelhana do
referido no EuroHeart Survey
(33)
; outros tipos de
IC foram menos frequentes, nomeadamente a IC
direita isolada e a IC multifactorial.
A demora mdia de internamento situou-se
dentro dos valores referidos para a IC na
Europa, por Stewart e cols (8 dias para os
homens, 10 para as mulheres), por Brown e
Cleland (11,3 dias, com grande variabilidade
conforme a patologia concomitante); j Wright e
cols, na Nova Zelndia apresentam 6 dias
(48)
.
Nos Estados Unidos da Amrica, o estudo
ADHERE mostrou uma demora mdia do
internamento de 4,5 dias, que estar em grande
parte relacionada com a existncia de
estruturas de cuidados continuados para onde
estes doentes so transferidos aps a alta
hospitalar; todavia, registou-se tambm uma
elevada taxa de re-internamento
(69)
. De referir
que, no EuroHeart Survey, a demora mdia do
internamento variou entre 7 e 19 dias, sendo
superior a 10 dias em 59% dos Pases includos
no estudo
(33)
. Numerosos factores influenciam o
tempo de internamento: mortalidade intra-
hospitalar, factores scio-demogrficos, taxa de
comorbilidade, qualidade do atendimento, tipo 24
stay: in-hospital mortality, sociodemographic
factors, rate of comorbidity, quality of care, type
of facility providing treatment and capacity for
care in the community, and health authorities
need to be made aware of these aspects.
In-hospital mortality was high, as is usually
found in patients with acute or chronic
decompensated HF
(9)
.
In conclusion, the present study identified
HF as the first cause of hospitalization in the
Medical Department of a teaching hospital in
an urban area, with an open external emergency
room, reflecting the true situation of patients
with acute HF admitted to hospital. As pointed
out in the ESC guidelines for acute or chronic
decompensated HF, treatment of such patients
should follow a program with a predefined
protocol in hospital departments that have their
own functional structures, under the guidance
of specialists in this area
(9)
. Various types of HF
clinics with day hospital facilities have already
proved that it is possible to give these patients
appropriate treatment at low cost and to reduce
rehospitalizations
(19, 27)
.
For the reasons given above, this patient
group requires a specialized, multidisciplinary
approach that involves physicians, nurses, diet-
itians, pharmacologists, physiotherapists and
social workers. Procedures should be
systematically defined in the departments
protocols to address the following needs:
prompt, accurate etiological and functional
diagnosis of the syndrome, identification of
comorbidities, initiation of appropriate therapy,
identification of social needs, preparation of the
outside environment to allow for early
discharge, and education of patients and their
families. In this way, we can achieve rapid
improvement in symptoms, greater compliance
with therapy, better and earlier identification of
factors triggering decompensation, and
reductions in length of hospital stay, in-hospital
and outpa-
tient morbidity and mortality, and
rehospitalization, which represents most of the
costs involved in this syndrome. As well as
specialized teams, it is essential to establish
physical structures such as day hospital and
continuing care facilities, which are certainly
less complex and costly than hospital admission
units.
Rev Port Cardiol
Vol. 25 Janeiro 01/January 01
ARTIGO 26-05-2006 15:26 Page 24
de estruturas que dispensam o tratamento,
capacidade de acolhimento na comunidade,
aspectos para os quais premente a
sensibilizao das entidades da sade.
A mortalidade intra-hospitalar foi elevada,
como habitualmente referido para doentes
com IC aguda ou crnica descompensada
(9)
.
Assim, em concluso, o presente estudo
identificou a IC como primeira causa de
internamento em departamento de medicina de
hospital com ensino, em rea urbana, com
urgncia externa aberta, reflectindo a realidade
da populao com IC aguda que acorre ao
hospital para internamento. Como salientado
nas recomendaes de IC aguda e crnica
agudizada, a assistncia aos doentes nesta fase
deve seguir uma programao pr-definida,
protocolada, em servios hospitalares com
estruturas funcionais prprias, devendo ser
orientado por Especialistas nesta rea
(9)
. Os
vrios tipos de clnicas de IC com hospital de
dia j deram provas de que possvel, com
baixo custo, assistir correctamente estes doen-
tes e reduzir a re-hospitalizao, aps a alta
(19,
27)
.
Pelas caractersticas atrs descritas, este
grupo de doentes necessita de uma abordagem
especializada e multidisciplinar, na qual
colaborem mdicos, enfermeiros, dietistas,
farmacuticos, fisioterapeutas, assistentes
sociais. Os procedimentos devero ser
sistematicamente protocolados nos Servios,
para responder s seguintes necessidades:
diagnstico da sndrome, etiolgico e funcional,
rpido e preciso, identificao de co-
morbilidades, instituio de teraputica
adequada, identificao de carncias sociais,
preparao do ambiente no exterior para a alta
precoce, educao do doente e seus familiares.
Assim podemos promover uma rpida melhoria
sintomtica, maior adeso teraputica,
identificao correcta e precoce dos factores de
descompensao, reduzir o tempo de
internamento, a morbi-mortalidade intra-
hospitalar e no ambulatrio e a readmisso
hospitalar, que consome a maior parte dos
custos envolvidos nesta sndrome. A par da
diferenciao das equipas, indispensvel a
criao de estruturas fsicas: Hospitais-de-Dia
e Cuidados Continuados, que so seguramente
menos complexas e dispendiosas do que as
Unidades de Internamento Hospitalar.
PEDRO MORAES SARMENTO, et al
Rev Port Cardiol 2006; 25: 13-27
Pedidos de separatas para:
Address for reprints:
PEDRO MORAES SARMENTO
Faculdade de Cincias Mdicas
Universidade Nova de Lisboa
Rua Prof. Mrio Albuquerque, 101, 4.-A
1600-812 LISBOA, PORTUGAL
e-mail: pmsarmento@netcabo.pt
ARTIGO 26-05-2006 15:26 Page 25
1. Reitsma J, Mosterd A, de Craen A, et al. Increase in
hospital admission rates for heart failure in the Netherlands,
1980-1993. Heart 1996;76:388-92.
2. Ni H, Naumann D, Hershberger R. Analysis of trends in
hospitalizations for heart failure. J Cardiac Fail 1999;5:79-84.
3. Stewart S, McIntyre K, MacLeod MM, Bailey AE, Capewell
S, McMurray JJV. Trends in hospitalization for heart failure
in Scotland 1990-1996. An epidemic that has reached its
peak. Eur Heart J 2001;22:209-17.
4. Redfield MM, Jacobsen SJ, Burnett JC Jr., Mahoney DW,
Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic
ventricular dysfunction in the community: appreciating the
scope of the heart failure epidemic. JAMA 2003;289:294-
-202.
5. Stewart S, McIntyre K, Capewell S, McMurray JJV. An
ageing population and heart failure: an increasing burden in
the 21st century? Heart 2003;89:40-53.
6. McMurray JJV, Petrie M, Murdoch D, Davie A. Clinical
epidemiology of heart failure: public and private health
burden. Eur Heart J 1998;19(Suppl P):P9-16.
7. Tavazzi L. Epidemiological burden of heart failure. Heart
1998:79(Suppl S): S6-9.
8. Stewart S, Jenkins A, Buschan S et al. The current cost of
heart failure in the UK - an economic analysis. Eur J Heart
Fail 2002;4:361-71.
9. Nieminem MS, Bohm M, Cowie MR, Drexler H, Filippatos
GS, Jondeau G et al. Executive summary of the guidelines on
the diagnosis and treatment of acute heart failure. The Task
Force on Acute Heart Failure of the European Society of
Cardiology. Eur Heart J 2005. Published ahead of print.
doi:10.1093/eurheartj/ehi044.
10. Ceia F, Fonseca C, Mota T, Morais H, Matias F, de Sousa
A, Gouveia-Oliveira A, on behalf of the EPICA Investigators.
Prevalence of chronic heart failure in Southwestern Europe:
the EPICA study. Eur J Heart Fail 2002;4:531-539.
11. Cleland JGF, Cohen-Solal A, Cosn Aguillar J, et al.
Management of heart failure in primary care (the
IMPROVEMENT of Heart Failure Programme): an
international survey. Lancet 2002;360:1631-1639.
12. Ceia F, Fonseca C, Azevedo I, Mota T, Morais H, Matias
F, Costa C, et al., on behalf of the EPICA-RAM investigators.
Epidemiology of heart failure in primary care in the
Autonomous Region of Madeira: the EPICA-RAM study. Rev
Port Cardiol 2005;24:173-189.
13. Fisher M, Baessler A, Hense HW, Hengstenberg C,
Muscholl M, Homer S, et al. Prevalence of left ventricular
diastolic dysfunction in the community: results from a
Doppler echocardiographic-based survey of a population
sample. Eur H J 2003;24:320-328.
14. Hogg K, Swedberg K, McMurray JJ. Heart failure with
preserved systolic function: epidemiology, clinical
characteristics, and prognosis. J Am Coll Cardiol
2004;43:317-327.
15. Ferreira A, Fernando PM, Cortez M, Capucho R, Brando
F, Cerqueira-Gomes M. Epidemiologic aspects of congestive
heart failure. Retrospective analysis of 2561 hospital
admissions. Rev Port Cardiol 1996;15:395-410.
16. Ceia F, Fonseca C, Mota T, Morais H, Matias F, Costa C,
Gouveia-Oliveira A, on behalf of the EPICA investigators.
Epidemiology of heart failure in mainland Portugal: New data
from the EPICA study. Rev Port Cardiol 2004;23(Suppl. III):
15-22.
17. Fonseca C, Morais H, Mota T, Matias F, Costa C,
Gouveia-Oliveira A, Ceia F. The diagnosis of heart failure in
primary care: value of symptoms and signs. Eur J Heart Fail
2004;6:795-800.
18. Wheeldon N, MacDonald T, Flucker CJ, McKendrick AD, 26
McDweitt D, Stuthers AD. Chronic heart failure in the
community: an echocardiographic study of its prevalence and
an assessment of the workload it generates for primary health
care and hospital physicians. Q J Med 1993;86:17-23.
19. Dahlstrm U. Frequent non-cardiac comorbidities in pa-
tients with chronic heart failure. Eur J Heart Fail 2005;7:
309-316.
20. Brown AM, Cleland JG. Influence of concomitant disease
on patterns of hospitalization in patients with heart failure
discharged from Scottish hospitals in 1995. Eur Heart J 1998;
19:1063-1069.
21. Martinez-Sells M, Robles JAG, Muoz R, Serrano JA,
Frades E, Muoa MD et al. Pharmacological treatment in pa-
tients with heart failure: patients knowledge and occurrence
of polypharmacy, alternative medicine and immunizations.
Eur J Heart Fail 2004;6:219-226.
22. Ledwidge M, Travers B, Ryder M, Ryan E, McDonald K.
Specialist care of heart failure improves appropriate
pharmacotherapy at the expense of greater polypharmacy and
drug-interactions. Eur J Heart Fail 2004;6:235-243.
23. Veehof L, Stewart R, Haaijer-Ruskamp F, Jong BM. The
development of polypharmacy. A longitudinal study. Fam
Pract June 2000;17:261-7.
24. Gustafsson F, Arnold JM. Heart failure clinics and
outpatient management: review of the evidence and call for
quality assurance. Eur Heart J 2004;25:1565-7.
25. Bocchi EA. Heart failure clinics: the Brazilian
experience. Rev Port Cardiol 2004;Suppl 3:III47-55.
26. Fonarow GC. Heart failure disease management programs.
Not a class effect. Circulation 2004;110:3506-3508.
27. Galbreath AD, Krasuski RA, Smith B, et al. Long-term
health care and cost outcomes of disease management in a
large, randomized, community-based population with heart
failure. Circulation 2004;110:3518-3526.
28. Phillips CO, Wright SM, Kern DE, Singa RM, Shepperd
S, Rubin HR. Comprehensive discharge planning with
postdischarge support for older patients with congestive heart
failure. JAMA 2004;291:1359-1367.
29. Task Force for the Diagnosis and Treatment of Chronic
Heart Failure, European Society of Cardiology: W. J. Remme
and K. Swedberg. Guidelines for the diagnosis and treatment
of chronic heart failure. Eur Heart J 2001;22:1527-1560.
30. A Report of the American College of
Cardiology/American Heart Association Task Force on
Practice Guidelines (Committee to Revise the 1995
Guidelines for the Evaluation and Management of Heart
Failure). ACC/AHA Guidelines for the evaluation and
management of chronic heart failure in the adult: executive
summary. Circulation 2001;104:2996-3007.
31. Ceia F, Fonseca C, Brito D, Madeira H. Heart failure
treatment in Portuguese hospitals: results of a survey. Rev
Port Cardiol 2001;20:1259-66.
32. Fonseca C, Ceia F, Brito D, Madeira H. How patients with
heart failure are managed in Portugal. Eur J Heart Fail 2002;
4:563-566.
33. Cleland JGF, Swedberg K, Follath F, Komadja M, Cohen-
Solal A, Aguilar JC et al. The EuroHeart failure survey
programme - a survey on the quality of care among patients
with heart failure in Europe. Part 1: patient characteristics
and diagnosis. Eur Heart J 2003;24:442-463.
34. Ceia F, Fonseca C, Mota T, Morais H, Matias F, Costa C,
Gouveia-Oliveira A. Aetiology, comorbidity and drug therapy
of chronic heart failure in the real world: the EPICA
substudy. Eur J Heart Fail 2004;6:801-806
35. Quiones MA, Waggoner AD, Reduto LA, Nelson JG,
Young JB, Winters, WL Jr. et al. A new, simplified and
accurate method for determining ejection fraction with two-
Rev Port Cardiol
Vol. 25 Janeiro 01/January 01
BIBLIOGRAFIA / REFERENCES
ARTIGO 26-05-2006 15:26 Page 26
dimensional echocardiography. Circulation 1981;744-53.
36. Dodge HT, Sandler H, Baxley WA, Hawley RR.
Usefulness and limitations of radiographic methods for
determining left ventricular volume. Am J Cardiol
1966;10:24.
37.Sandler H, Dodge HT. The use of single plane
angiocardiograms for the calculation of left ventricular volume
in man. Am Heart J 1968;325:34.
38. Imaging Guidelines for Nuclear Cardiology Procedures.
American Society of Nuclear Cardiology. Equilibrium gated
blood pool imaging protocols. J Nucl Cardiol 1996;26-9.
39. Henry WL, deMaria A, Gramiak R et al. Report of the
American Society of Echocardiography Committee on
nomenclature and standards in two-dimensional echocardi-
ography. Circulation 1980;62:212-7.
40. Bonow RO, Carabello B, de Leon AC, Edmunds LH Jr.,
Fedderly BJ, Freed MD et al. ACC/AHA Guidelines for the
Management of Patients With Valvular Heart Disease.
Executive Summary. A report of the American College of
Cardiology/American Heart Association Task Force on
Practice Guidelines (Committee on Management of Patients
with Valvular Heart Disease). J Heart Valve Dis 1998;672-
677.
41. American Diabetes Association. Summary of revisions for
the 2004 Clinical Practice Recommendations. Diabetes Care
2004;27:suppl. I.
42. Brito D, Pedro M, Metrass MJ, Pdua F, Madeira H. Heart
failure: diastolic dysfunction vs. systolic dysfunction. Rev
Port Cardiol 1995;14:741-4.
43. Martinez-Sells M, Robles JAG, Prieto L, Serrano JA,
Muoz R, Frades E, Almendral J. Annual rates of admission
and seasonal variations in hospitalizations for heart failure.
Eur J Heart Fail 2002;4:779-786.
44. Grupo de Trabajo de Insuficiencia Cardiaca de la
Sociedad Espaola de Medicina Interna. Heart failure in
internal medicine departments. Med Clin (Barc)
2002;118:605-610.
45. Wright SP, Verouhis D, Gamble G, Swedberg K, Sharpe
N, Doughty RN. Factors influencing the length of hospital
stay of patients with heart failure. Eur J Heart Fail 2003;5:
201-209.
46. Di Lenarda A, Scherillo M, Maggioni AP, Acquarone N,
Ambrosio GB, Annichiarico M, et al. Current presentation
and management of heart failure in cardiology and internal
medicine hospital units: a tale of two worlds - the
TEMISTOCLE study. Am Hear J 2003; 146: e12.
doi:10.1016/s0002-8703(03)00315-6.
47. Ho KKL, Pinsky JL, Kannel WB, Levy D. The
epidemiology of heart failure: the Framingham study. J Am
Coll Cardiol 1993;22 (suppl A):6A-13A.
48. Braunstein JB, Anderson GF, Gerstenblith G, Weller W,
Niefeld M, Herbert R, et al. Noncardiac comorbidity
increases preventable hospitalizations and mortality among
Medicare beneficiaries with chronic heart failure. J Am Coll
Cardiol 2003;42:1226-1233.
49. Macedo ME, Lima MJ, Silva AO, Alcntara P, Carmona J.
Prevalence, awareness, treatment and control of hypertension in
Portugal. J Hypertension 2005. J Hypertens 2005;23:1661-6.
50. Moraes-Sarmento P, Marques F, Fonseca C.
Hipocoagulao oral na profilaxia do acidente
tromboemblico: normas prticas de actuao. RFML
2002;7:287-97.
51. The sixth ACCP Consensus Conference on Antithrombotic
Therapy. Chest 2001;119:194S-206S.
52. Ogren M, Bergqvist D, Eriksson H, Lindblad B, Sternby
NH. Prevalence and risk of pulmonary embolism in patients
with intracardiac thrombosis: a population-based study of 23
796 consecutive autopsies. Eur Heart J 2005;4 Feb. Epub-
ahead-of-print.
53. Rosenow EC 3rd. Venous and pulmonary
thromboembolism: an algorithmic approach to diagnosis and
treatment. Mayo Clin Proc 2005;70:5067.
54. Van der Wal MHL, Jaarsma T, van Veldhuisen DJ. Non-
compliance in patients with heart failure: how can we manage
it? Eur J Heart Fail 2005;7:5-18.
55. Kannel WB, McGee DL. Diabetes and glucose tolerance
as risk factors for cardiovascular disease: the Framingham
study. Diabetes Care 1979;2:120-126.
56. Dries DL, Sweitzer NK, Drazner MH, Stevenson LW,
Gersh BJ. Prognostic impact of diabetes mellitus in patients
with heart failure according to the etiology of left ventricular
systolic dysfunction. J Am Coll Cardiol 2001;38:421-428.
57. De Groote P, Lamblin N, Mouquet F, Plichon N,
McFadden E, Van Belle F, et al. Impact of diabetes mellitus
on long-term survival in patients with congestive heart failure.
Eur Heart J 2004;25:256-62.
58. Ezekowitz JA, McAlister FA, Armstrong PW. Anemia is
common in heart failure and is associated with poor outcomes:
insights from a cohort of 12065 patients with new onset heart
failure. Circulation 2003;197:223-225.
59. Maggioni AP, Opasich C, Anand I, et al. Anemia in pa-
tients with heart failure: prevalence and prognostic role in a
controlled trial and in clinical practice. J Card Fail 2005;11:
91-98.
60. Horwich TB, Fonarow GC, Hamilton MA, MacLellan WR,
Borensten A. Anemia is associated with worse symptoms,
greater impairment of functional capacity and a significant
increase in mortality in patients with advanced heart failure. J
Am Coll Cardiol 2002;39:1780-1786.
61. McCullough PA, Lepor NE. The deadly triangle of
anemia, renal insufficiency, and cardiovascular disease:
implications for prognosis and treatment. Rev Cardiovasc
Med. 2005; 6:1-10.
62. Silverberg DS, Wexler D, Iaina A. The importance of
anemia and its correction in the management of severe
congestive heart failure. Eur J Heart Fail 2002;4:681-686.
63. Silverberg D, Wexler D, Blum M, Scwartz D, Iaina A. The
association between congestive heart failure and chronic
renal disease. Curr Opin Nephrol Hypertens 2004;13:163-70.
64. Bongartz LG, Cramer MJ, Doevendans PA, Joles JA,
Braam B. The severe cardiorenal syndrome: Guyton
revisited. Eur Heart J 2005;26:11-7.
65. McCullough PA, Hollander JE, Nowak RM, Storrow AB,
Duc P, Om T, et al. Uncovering heart failure in patients with
a history of pulmonary disease: rationale for the early use of
B-type natriuretic peptide in the emergency department.
Acad Emerg Med 2003;10:198-204.
66. Salpeter SR, Ormiston TM, Salpeter EE. Cardioselective
beta-blockers in patients with reactive airway disease: a
meta-analysis. Ann Inern Med 2002;137:715-725.
67. Jones RC, Francis GS, Lauer MS. Predictors of mortality
in patients with heart failure and preserved systolic function
in the Digitalis Investigation Group trial. J Am Coll Cardiol
2004;44:1025-9.
68. Lenzen MJ, Scholte op Reimer WJM, Boersma E,
Vantrimpont PJMJ, Follath F, Swedberg K, Cleland J,
Komadja M. Differences between patients with a preserved
and a depressed left ventricular function: a report from the
EuroHeart Failure Survey. Eur Heart J 2004;25:1214-1220.
69. Fonarow GC, for the ADHERE Scientific Advisory
Committee. Heart Failure Reviews 2004;9:179-185.
PEDRO MORAES SARMENTO, et al
Rev Port Cardiol 2006; 25: 13-27
ARTIGO 26-05-2006 15:26 Page 27
Vous aimerez peut-être aussi
- Fundamentos Da EnfermagemDocument128 pagesFundamentos Da Enfermagemrico.ferr97% (112)
- Material de Apoio PulsologiaDocument9 pagesMaterial de Apoio PulsologiaGuga GalanoPas encore d'évaluation
- 1° SocorrosDocument14 pages1° SocorrosGlaydson ReisPas encore d'évaluation
- Medicamentos em PediatriaDocument89 pagesMedicamentos em PediatriaEnfermagemFaternPas encore d'évaluation
- Prova Pratica Histologia II - EREDocument15 pagesProva Pratica Histologia II - EREVítor GonzagaPas encore d'évaluation
- Sinais Vitais PDFDocument52 pagesSinais Vitais PDFDébora RibeiroPas encore d'évaluation
- #1 Broken by Lies - Bound and Broken - Rebecca SheaDocument213 pages#1 Broken by Lies - Bound and Broken - Rebecca SheaRobson RiegerPas encore d'évaluation
- AIDPI para o Ensino MédicoDocument74 pagesAIDPI para o Ensino MédicoEnfermagemFaternPas encore d'évaluation
- Terminologia Médica PDFDocument25 pagesTerminologia Médica PDFrafael freirePas encore d'évaluation
- Teste SangueDocument4 pagesTeste Sangueyves raphael100% (1)
- Tabela para Preparo e Administração de Medicamentos Injetáveis SF HU Unidades NeonataisDocument23 pagesTabela para Preparo e Administração de Medicamentos Injetáveis SF HU Unidades NeonataisEnfermagemFaternPas encore d'évaluation
- Prova e Chave de Respostas - Area 2 - Fisiologia Bioquimica e Exercicio 0Document11 pagesProva e Chave de Respostas - Area 2 - Fisiologia Bioquimica e Exercicio 0GustavoPas encore d'évaluation
- Amiodarona OralDocument14 pagesAmiodarona OralMarta ViolantePas encore d'évaluation
- Meridiano Da Bexiga MTCDocument37 pagesMeridiano Da Bexiga MTCCarol GnoattoPas encore d'évaluation
- Aula de Cardiopatia Congênita Pós GraduaçãoDocument85 pagesAula de Cardiopatia Congênita Pós GraduaçãoMarco RoquePas encore d'évaluation
- Fisiologia Do Sistema CardiovascularDocument21 pagesFisiologia Do Sistema CardiovascularFernanda AmaralPas encore d'évaluation
- (LAUDO - DS) (ECG) (ECG Demissional) (JEERSON BRUNO SOUZA DE JESUS) (28A) (3302906) (20230320120343)Document1 page(LAUDO - DS) (ECG) (ECG Demissional) (JEERSON BRUNO SOUZA DE JESUS) (28A) (3302906) (20230320120343)andreza andrade limaPas encore d'évaluation
- Bula DorflexUNODocument22 pagesBula DorflexUNOwilson ferrariPas encore d'évaluation
- OSCE P3 by CACIQUE-ALMIRANTE-MADEIRADocument3 pagesOSCE P3 by CACIQUE-ALMIRANTE-MADEIRAThawany MouraPas encore d'évaluation
- Acesso Venoso CentralDocument7 pagesAcesso Venoso CentralCarolina Poblete Urrutia HarmbacherPas encore d'évaluation
- Manual de Siglas e Abreviaturas MédicasDocument56 pagesManual de Siglas e Abreviaturas Médicasdell_AllFunPas encore d'évaluation
- Projeto PNI-Oximetro PDFDocument126 pagesProjeto PNI-Oximetro PDFWagner PagotoPas encore d'évaluation
- Prova Final Ciencias 5 AnoDocument6 pagesProva Final Ciencias 5 AnoVanemoremaffePas encore d'évaluation
- Exercícios Sistema CardiovascularDocument3 pagesExercícios Sistema CardiovascularHenrique AraujoPas encore d'évaluation
- Emergencias Na Anestesia VeterinariaDocument5 pagesEmergencias Na Anestesia VeterinariaAle AlssufePas encore d'évaluation
- MÚSCULOSDocument8 pagesMÚSCULOSArlete Ernestina lima100% (1)
- A Circulação Do Sangue e Distribuição de Líquidos Se Dá Pela Ação Bombeadora Do CoraçãoDocument4 pagesA Circulação Do Sangue e Distribuição de Líquidos Se Dá Pela Ação Bombeadora Do Coraçãopamcos15Pas encore d'évaluation
- 8 Série - Prova de FisiologiaDocument4 pages8 Série - Prova de FisiologiaNízia PortoPas encore d'évaluation
- 201 242 Ciencias 8 Ano Vol2 2020Document40 pages201 242 Ciencias 8 Ano Vol2 2020margarida mangabeiraPas encore d'évaluation
- 2cuidados Paliativos em Geriatria ApostilaDocument41 pages2cuidados Paliativos em Geriatria ApostilajuliaPas encore d'évaluation
- 01-Classe Das AvesDocument43 pages01-Classe Das AvesACORDE AGORA SAIA DA MATRIXPas encore d'évaluation
- Lista de Biologia - Exercícios ObrigatóriosDocument32 pagesLista de Biologia - Exercícios ObrigatóriosluciPas encore d'évaluation
- Casos Clinicos - LAECCDocument3 pagesCasos Clinicos - LAECCAnderson filhoPas encore d'évaluation
- Lesões Valvares Mitrais e Tricuspides - Semiologia ClínicaDocument31 pagesLesões Valvares Mitrais e Tricuspides - Semiologia ClínicaFernando SantannaPas encore d'évaluation