Vous aimerez peut-être aussi
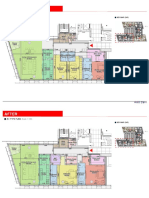
- Before: A1 Type PlanDocument2 pagesBefore: A1 Type PlanNgoc Vũ TrầnPas encore d'évaluation
- Technical CataloguelDocument20 pagesTechnical CataloguelNgoc Vũ TrầnPas encore d'évaluation
- Important PDFDocument1 pageImportant PDFNgoc Vũ TrầnPas encore d'évaluation
- Solar System SpecDocument23 pagesSolar System SpecNgoc Vũ TrầnPas encore d'évaluation
- Vcc-Mep Value Engineer Approved - To CTCDocument1 pageVcc-Mep Value Engineer Approved - To CTCNgoc Vũ TrầnPas encore d'évaluation
- APV HE Leo DuraFlow 1214 02 04 2012 GBDocument2 pagesAPV HE Leo DuraFlow 1214 02 04 2012 GBNgoc Vũ TrầnPas encore d'évaluation
- Pheu Thu San-Ngoc ThaoDocument1 pagePheu Thu San-Ngoc ThaoNgoc Vũ TrầnPas encore d'évaluation
- AHU-B01-04 All Day Dining-Cooling PDFDocument1 pageAHU-B01-04 All Day Dining-Cooling PDFNgoc Vũ TrầnPas encore d'évaluation
- AHU-B01-04 All Day Dining-Heating PDFDocument1 pageAHU-B01-04 All Day Dining-Heating PDFNgoc Vũ TrầnPas encore d'évaluation
- Electro-Mechanical Room Thermostat For Thermal ActuatorsDocument4 pagesElectro-Mechanical Room Thermostat For Thermal ActuatorsNgoc Vũ TrầnPas encore d'évaluation
- tbn001 PDFDocument1 pagetbn001 PDFNgoc Vũ TrầnPas encore d'évaluation
- Control of Air Pollution in Car Parks PDFDocument7 pagesControl of Air Pollution in Car Parks PDFNgoc Vũ TrầnPas encore d'évaluation
- Sound PDFDocument4 pagesSound PDFNgoc Vũ TrầnPas encore d'évaluation
- Fan Terminology and Definitions: Technical Bulletin TBN002.2/2003Document4 pagesFan Terminology and Definitions: Technical Bulletin TBN002.2/2003Ngoc Vũ TrầnPas encore d'évaluation
- Cycle of Concentration in Cooling Tower PDFDocument1 pageCycle of Concentration in Cooling Tower PDFNgoc Vũ TrầnPas encore d'évaluation
- Trane - Wall Mounted FCU PDFDocument2 pagesTrane - Wall Mounted FCU PDFNgoc Vũ TrầnPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Vibration Absorbers: Scan This QR CodeDocument4 pagesVibration Absorbers: Scan This QR CodeMohamed RaafatPas encore d'évaluation
- EWC 662 English Writing Critical Group Work Portfolio: Submitted ToDocument31 pagesEWC 662 English Writing Critical Group Work Portfolio: Submitted ToNurul Nadia MuhamadPas encore d'évaluation
- Effect of Different Laser Texture Configurations On Improving Surface Wettability and Wear Characteristics of Ti6Al4V Implant MaterialDocument14 pagesEffect of Different Laser Texture Configurations On Improving Surface Wettability and Wear Characteristics of Ti6Al4V Implant Materialnitish kumar100% (1)
- Alma Matter SpeechDocument1 pageAlma Matter Speechlariza gallegoPas encore d'évaluation
- Generic NdaDocument2 pagesGeneric NdalataminvestmentsPas encore d'évaluation
- Syllabus Financial AccountingDocument3 pagesSyllabus Financial AccountingHusain ADPas encore d'évaluation
- Debit Note and Credit NoteDocument2 pagesDebit Note and Credit Noteabdul haseebPas encore d'évaluation
- Banking Adbl EnglishDocument74 pagesBanking Adbl Englishdevi ghimirePas encore d'évaluation
- Four Quartets: T.S. EliotDocument32 pagesFour Quartets: T.S. Eliotschwarzgerat00000100% (1)
- Recruitment of Officers in Grade B' (General) - DR - By-2019Document2 pagesRecruitment of Officers in Grade B' (General) - DR - By-2019Shalom NaikPas encore d'évaluation
- Harmonica IntroDocument5 pagesHarmonica Introapi-26593142100% (1)
- A Simple and Reliable Submental Intubation.68Document4 pagesA Simple and Reliable Submental Intubation.68Tîrban Pantelimon FlorinPas encore d'évaluation
- 16.3 - Precipitation and The Solubility Product - Chemistry LibreTextsDocument14 pages16.3 - Precipitation and The Solubility Product - Chemistry LibreTextsTherePas encore d'évaluation
- Proposal Mini Project SBL LatestDocument19 pagesProposal Mini Project SBL Latestapi-310034018Pas encore d'évaluation
- Everyday Life - B1 - ShoppingDocument7 pagesEveryday Life - B1 - ShoppingAmi BarnesPas encore d'évaluation
- Fruit Brearing CropsDocument177 pagesFruit Brearing CropsJoshua G. Sapin100% (1)
- KC CVDocument2 pagesKC CVVishal KeshriPas encore d'évaluation
- Getting Things Done BasicsDocument60 pagesGetting Things Done Basicswestelm12100% (10)
- DLL English 7-10, Week 1 Q1Document8 pagesDLL English 7-10, Week 1 Q1Nemfa TumacderPas encore d'évaluation
- Factors Influencing The Selection Of: MaterialsDocument22 pagesFactors Influencing The Selection Of: MaterialsMaulik KotadiyaPas encore d'évaluation
- TV ExplorerDocument2 pagesTV Explorerdan r.Pas encore d'évaluation
- Congenital Abnormalities of The Female Reproductive TractDocument14 pagesCongenital Abnormalities of The Female Reproductive TractMary SheshiraPas encore d'évaluation
- Nursing ManagementDocument5 pagesNursing Managementheron_bayanin_15Pas encore d'évaluation
- Flexure Hinge Mechanisms Modeled by Nonlinear Euler-Bernoulli-BeamsDocument2 pagesFlexure Hinge Mechanisms Modeled by Nonlinear Euler-Bernoulli-BeamsMobile SunPas encore d'évaluation
- InvoiceDocument1 pageInvoiceKidambi SureshPas encore d'évaluation
- What Is NanoWatt TechnologyDocument1 pageWhat Is NanoWatt Technologyfolk_sharathPas encore d'évaluation
- ShowimgDocument76 pagesShowimgROSHAN ROBERTPas encore d'évaluation
- 2015.15009.fundamental Principles of Physical Chemistry - Text PDFDocument782 pages2015.15009.fundamental Principles of Physical Chemistry - Text PDFAnoif Naputo Aidnam100% (1)
- Lotte Advanced Materials Co., LTD.: ISO 9001:2015, KS Q ISO 9001:2015Document2 pagesLotte Advanced Materials Co., LTD.: ISO 9001:2015, KS Q ISO 9001:2015Tayyab KhanPas encore d'évaluation
- Caribbean Career Opportunity - Cayman Island Water Authority - Plant Operator Cayman Brac Plant Operator (Overseas)Document1 pageCaribbean Career Opportunity - Cayman Island Water Authority - Plant Operator Cayman Brac Plant Operator (Overseas)Cawasa St-LuciaPas encore d'évaluation