Vous aimerez peut-être aussi
- Gastric CancerDocument25 pagesGastric CancerAndreea SubcinschiPas encore d'évaluation
- Epidemiology, Pathogenesis, and Clinical Manifestations of Celiac Disease in Children - UpToDateDocument26 pagesEpidemiology, Pathogenesis, and Clinical Manifestations of Celiac Disease in Children - UpToDatejandagashvili2007Pas encore d'évaluation
- Acanthosis Nigricans - emedICINE.2012.2013.FCPSDocument16 pagesAcanthosis Nigricans - emedICINE.2012.2013.FCPSAbdul QuyyumPas encore d'évaluation
- Akne Obese Lipid 2009Document5 pagesAkne Obese Lipid 2009Henyta TsuPas encore d'évaluation
- Diabetes Hypertension Obesity: PathophysiologyDocument3 pagesDiabetes Hypertension Obesity: PathophysiologyDevy AndikaPas encore d'évaluation
- SJ Ijo 0800495Document23 pagesSJ Ijo 0800495Mohammad shaabanPas encore d'évaluation
- The Metabolic Syndrome in Polycystic Ovary SyndromeDocument21 pagesThe Metabolic Syndrome in Polycystic Ovary SyndromeHAVIZ YUADPas encore d'évaluation
- Type 2 Diabetes Mellitus - Prevalence and Risk Factors - UpToDateDocument36 pagesType 2 Diabetes Mellitus - Prevalence and Risk Factors - UpToDateEver LuizagaPas encore d'évaluation
- Approach To The Patient With Unintentional Weight LossDocument11 pagesApproach To The Patient With Unintentional Weight LossPetru-Emanuel DascalitaPas encore d'évaluation
- Sam CD Diabetes MellitusDocument26 pagesSam CD Diabetes MellitusDr. Muha. Hasan Mahbub-Ur-RahmanPas encore d'évaluation
- Comorbidities and Complications of Obesity in Children and Adolescents - UpToDateDocument35 pagesComorbidities and Complications of Obesity in Children and Adolescents - UpToDatemarina alvesPas encore d'évaluation
- Preamble: Podcast Interview: - Also Available On ItunesDocument18 pagesPreamble: Podcast Interview: - Also Available On ItuneswawanpecelPas encore d'évaluation
- Insulin OmaDocument17 pagesInsulin OmaRezky Faried HidayatullahPas encore d'évaluation
- Ovario Poliquistico Articulo 2011Document16 pagesOvario Poliquistico Articulo 2011nikonhpPas encore d'évaluation
- 1 s2.0 S0026049517302743 MainDocument11 pages1 s2.0 S0026049517302743 MainTeodora OnofreiPas encore d'évaluation
- Epidemiology and Pathophysiology of Colonic Diverticular DiseaseDocument8 pagesEpidemiology and Pathophysiology of Colonic Diverticular DiseaseAnonymous Hz5w55Pas encore d'évaluation
- Fatty Pancreas Clinical ImplicationsDocument6 pagesFatty Pancreas Clinical ImplicationsEngin ALTINTASPas encore d'évaluation
- Changing Trends in Peptic Ulcer Prevalence in A Tertiary Care Setting in The PhilippinesDocument3 pagesChanging Trends in Peptic Ulcer Prevalence in A Tertiary Care Setting in The PhilippinesRumelle ReyesPas encore d'évaluation
- Gestational Diabetes Mellitus: Science in MedicineDocument7 pagesGestational Diabetes Mellitus: Science in MedicineNatalia_p_mPas encore d'évaluation
- Hígado Graso No AlcohólicoDocument16 pagesHígado Graso No AlcohólicoAntonio Martinez GarciaPas encore d'évaluation
- Tugas Bahasa IndonesiaDocument26 pagesTugas Bahasa IndonesiaAtha KudmasaPas encore d'évaluation
- 4 Metabolic Complications Pedersen2013 - Alan OsorioDocument15 pages4 Metabolic Complications Pedersen2013 - Alan Osoriomtz.c.erikaPas encore d'évaluation
- Periodontal Infection and Glycemic Control in Diabetes: Current EvidenceDocument5 pagesPeriodontal Infection and Glycemic Control in Diabetes: Current EvidencegarciamanuelPas encore d'évaluation
- POSITION STATEMENTPreDMsop TRTRDocument12 pagesPOSITION STATEMENTPreDMsop TRTRTony CoaPas encore d'évaluation
- Obesity - StatPearls - NCBI BookshelfDocument8 pagesObesity - StatPearls - NCBI BookshelfWidad SalsabilaPas encore d'évaluation
- j.1365 2796.2006.01752.x20160829 29101 n3bfks With Cover Page v2Document12 pagesj.1365 2796.2006.01752.x20160829 29101 n3bfks With Cover Page v2herondalePas encore d'évaluation
- Reviews: Hyperinsulinaemia in CancerDocument16 pagesReviews: Hyperinsulinaemia in CancerThiago SartiPas encore d'évaluation
- Eating Disorders, Bulimia, AnorexiaDocument48 pagesEating Disorders, Bulimia, AnorexiaMariaPas encore d'évaluation
- Colonic Diverticulosis and Diverticular Disease Epidemiology, RiskDocument20 pagesColonic Diverticulosis and Diverticular Disease Epidemiology, RiskmohammedPas encore d'évaluation
- Pe Project Obesity: Name: Manas Kadam Class: XII A Commerce Roll No - 87Document32 pagesPe Project Obesity: Name: Manas Kadam Class: XII A Commerce Roll No - 87sahilPas encore d'évaluation
- Eating Pathology in Adolescents With Celiac Disease PDFDocument8 pagesEating Pathology in Adolescents With Celiac Disease PDFFrancisco ChristianPas encore d'évaluation
- NASH in ChildrenDocument10 pagesNASH in ChildrendrtpkPas encore d'évaluation
- Nutrients 05 02019Document9 pagesNutrients 05 02019FITYOURBODYPas encore d'évaluation
- Effect of Diet On Type 2 Diabetes MellitusDocument14 pagesEffect of Diet On Type 2 Diabetes MellitusPriya bhattiPas encore d'évaluation
- 2015 Sup 11 FullDocument5 pages2015 Sup 11 FullsebastianPas encore d'évaluation
- Obesityasadisease: Jagriti Upadhyay,, Olivia Farr,, Nikolaos Perakakis,, Wael Ghaly,, Christos MantzorosDocument21 pagesObesityasadisease: Jagriti Upadhyay,, Olivia Farr,, Nikolaos Perakakis,, Wael Ghaly,, Christos MantzorosAlejandra RamirezPas encore d'évaluation
- Definitions, Epidemiology, and Risk Factors For Inflammatory Bowel Disease - UpToDateDocument25 pagesDefinitions, Epidemiology, and Risk Factors For Inflammatory Bowel Disease - UpToDateTurma A 2019.1 Med-FCMPas encore d'évaluation
- Pe Project: Name: Aakanksh Biswas Class: XII A Commerce Roll No - 27Document28 pagesPe Project: Name: Aakanksh Biswas Class: XII A Commerce Roll No - 27sahilPas encore d'évaluation
- Summary of Andrew J. Wakefield's Waging War On The Autistic ChildD'EverandSummary of Andrew J. Wakefield's Waging War On The Autistic ChildPas encore d'évaluation
- Anorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDateDocument11 pagesAnorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDateAlejandra GarcíaPas encore d'évaluation
- The Relation of Overweight To Cardiovascular Risk Factors Among Children and Adolescents: The Bogalusa Heart StudyDocument10 pagesThe Relation of Overweight To Cardiovascular Risk Factors Among Children and Adolescents: The Bogalusa Heart StudyaocuPas encore d'évaluation
- Ulcerative Colitis in ChildrenDocument5 pagesUlcerative Colitis in ChildrentheservantPas encore d'évaluation
- البحثDocument43 pagesالبحثحسين علي ذيبان عليPas encore d'évaluation
- Diagnosis of Polycystic Ovary Syndrome in Adults - UpToDateDocument27 pagesDiagnosis of Polycystic Ovary Syndrome in Adults - UpToDatepeishanwang90Pas encore d'évaluation
- Pediatric Obesity and Gallstone Disease.18Document6 pagesPediatric Obesity and Gallstone Disease.18Merari Lugo OcañaPas encore d'évaluation
- Ovario Poliquístico/Polycystic Ovary SyndromeDocument14 pagesOvario Poliquístico/Polycystic Ovary SyndromeJosé María Lauricella100% (1)
- Dyslipidemia Journal ArticleDocument10 pagesDyslipidemia Journal ArticleJeanPas encore d'évaluation
- 2004 Metabolic Risk During Antipsychotic TreatmentDocument11 pages2004 Metabolic Risk During Antipsychotic TreatmentDiego HormacheaPas encore d'évaluation
- Gut-2006-Van Heel-1037-46Document11 pagesGut-2006-Van Heel-1037-46Codruta StanPas encore d'évaluation
- Type1 DiabetesDocument7 pagesType1 DiabetesbettyborblePas encore d'évaluation
- Colonic Diverticulosis and Diverticular Disease - Epidemiology, Risk Factors, andDocument25 pagesColonic Diverticulosis and Diverticular Disease - Epidemiology, Risk Factors, andBryan JimenezPas encore d'évaluation
- Waist and Hip Circumferences and Waist-Hip Ratio I-2Document1 pageWaist and Hip Circumferences and Waist-Hip Ratio I-2VenkatPas encore d'évaluation
- Metabolic Syndrome and StrokeDocument5 pagesMetabolic Syndrome and StrokeEmir SaricPas encore d'évaluation
- Anorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDateDocument10 pagesAnorexia Nervosa in Adults and Adolescents - The Refeeding Syndrome - UpToDatethelesphol pascalPas encore d'évaluation
- Best Practice & Research Clinical Endocrinology & MetabolismDocument11 pagesBest Practice & Research Clinical Endocrinology & MetabolismM Slamet RiyantoPas encore d'évaluation
- Eating Disorders - Overview of Epidemiology, Clinical Features, and Diagnosis - UpToDateDocument39 pagesEating Disorders - Overview of Epidemiology, Clinical Features, and Diagnosis - UpToDateDylanPas encore d'évaluation
- Diabetes Treatment Literature ReviewDocument7 pagesDiabetes Treatment Literature Reviewafmzatvuipwdal100% (1)
- Review of LiteratureDocument3 pagesReview of LiteraturepremPas encore d'évaluation
- ReflubDocument20 pagesReflubcantantederockPas encore d'évaluation
- Clinical Manifestations and Complications of Inflammatory Bowel Disease in Children and AdolescentsDocument926 pagesClinical Manifestations and Complications of Inflammatory Bowel Disease in Children and AdolescentsFlorin Calin LungPas encore d'évaluation
- Impact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyD'EverandImpact of Polycystic Ovary, Metabolic Syndrome and Obesity on Women Health: Volume 8: Frontiers in Gynecological EndocrinologyPas encore d'évaluation
- Ambulatory Blood Pressure Monitoring in Children - UpToDateDocument17 pagesAmbulatory Blood Pressure Monitoring in Children - UpToDateZeliha TürksavulPas encore d'évaluation
- An Approach To The Patient With Drug Allergy - UpToDateDocument26 pagesAn Approach To The Patient With Drug Allergy - UpToDateZeliha TürksavulPas encore d'évaluation
- Allergic Rhinitis Clinical Manifestations Epidemiology and DDocument23 pagesAllergic Rhinitis Clinical Manifestations Epidemiology and DZeliha TürksavulPas encore d'évaluation
- Allergic Reactions To Vaccines - UpToDateDocument23 pagesAllergic Reactions To Vaccines - UpToDateZeliha TürksavulPas encore d'évaluation
- Allergic Reactions To Vaccines - UpToDateDocument23 pagesAllergic Reactions To Vaccines - UpToDateZeliha TürksavulPas encore d'évaluation
- Acute Liver Failure in Children Management - UpToDateDocument20 pagesAcute Liver Failure in Children Management - UpToDateZeliha TürksavulPas encore d'évaluation
- FINAL Standalone Pediatric Obesity GuidelineDocument44 pagesFINAL Standalone Pediatric Obesity GuidelineZeliha TürksavulPas encore d'évaluation
- Acquired Torticollis in Children - UpToDateDocument21 pagesAcquired Torticollis in Children - UpToDateZeliha TürksavulPas encore d'évaluation
- Acquired Inhibitors of Coagulation - UpToDateDocument23 pagesAcquired Inhibitors of Coagulation - UpToDateZeliha TürksavulPas encore d'évaluation
- Efficacy and Safety of Prophylactic Vaccines Against Cervical HPV Infection andDocument31 pagesEfficacy and Safety of Prophylactic Vaccines Against Cervical HPV Infection andZeliha TürksavulPas encore d'évaluation
- Surgery Mcqs Along With KeyDocument8 pagesSurgery Mcqs Along With KeyFaizan Khan100% (3)
- KD 3.4 Reading Practice - Analytical ExpositionDocument6 pagesKD 3.4 Reading Practice - Analytical ExpositionManusiaa HiduppPas encore d'évaluation
- Uses of X-Rays in Medical FieldDocument6 pagesUses of X-Rays in Medical FieldShwe Pwint Pyae SonePas encore d'évaluation
- IMMUNOCAL Projected To Become #1Document2 pagesIMMUNOCAL Projected To Become #1m_wfulton3815Pas encore d'évaluation
- Zoladex 3.6mg Implant - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document8 pagesZoladex 3.6mg Implant - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)KunalPas encore d'évaluation
- Gout Diet Foods To Avoid and Low-Purine Foods To Eat InsteadDocument1 pageGout Diet Foods To Avoid and Low-Purine Foods To Eat InsteadDesiree Jolly Dela CruzPas encore d'évaluation
- OB-GYN - Standardized Patient PrepDocument6 pagesOB-GYN - Standardized Patient Prepskeebs23Pas encore d'évaluation
- CHEMOTHERAPYDocument28 pagesCHEMOTHERAPYDwi CahyaPas encore d'évaluation
- Fda Approved Contrast AgentsDocument55 pagesFda Approved Contrast AgentsPoojaSolankiPas encore d'évaluation
- Case Study For Colorectal CancerDocument23 pagesCase Study For Colorectal CancerAnjanette ViloriaPas encore d'évaluation
- For Oral CancerDocument88 pagesFor Oral Cancercjane.correos25Pas encore d'évaluation
- Brain Tumors (Benign and Malignant) - Symptoms, Causes, TreatmentDocument4 pagesBrain Tumors (Benign and Malignant) - Symptoms, Causes, TreatmentThuvija DarshiniPas encore d'évaluation
- Ferrets Oncology-MainDocument26 pagesFerrets Oncology-MainJOAQUINALONZOPEREIRAPas encore d'évaluation
- Qualitative Studies On Working Students 2Document75 pagesQualitative Studies On Working Students 2Angelica MatullanoPas encore d'évaluation
- LIC - Cancer Cover - Brochure - 9 Inch X 8 Inch - Eng - Single PagesDocument10 pagesLIC - Cancer Cover - Brochure - 9 Inch X 8 Inch - Eng - Single PagesKumar KalyanPas encore d'évaluation
- What Is Radioactive PollutionDocument4 pagesWhat Is Radioactive PollutionJoy MitraPas encore d'évaluation
- Group 10Document12 pagesGroup 10Esdras DountioPas encore d'évaluation
- 2015 Oncology CREOG Review PDFDocument76 pages2015 Oncology CREOG Review PDFRima HajjarPas encore d'évaluation
- AstrositomaDocument29 pagesAstrositomaFitria NurulfathPas encore d'évaluation
- AIChE Journal Vol (1) - 51 No. 12 December 2005Document229 pagesAIChE Journal Vol (1) - 51 No. 12 December 2005naraNJORPas encore d'évaluation
- Clinical Oncology PaperDocument20 pagesClinical Oncology Paperapi-633111194Pas encore d'évaluation
- 4 Interview Transcripts From The Anti Cancer Revolution 2Document72 pages4 Interview Transcripts From The Anti Cancer Revolution 2Pierre Le GrandePas encore d'évaluation
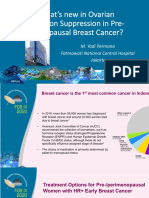
- 2.3.a DR Yadi Permana Whats New in Ovarian Function Suppression in Pre-MenopausalDocument36 pages2.3.a DR Yadi Permana Whats New in Ovarian Function Suppression in Pre-Menopausaltepat rshsPas encore d'évaluation
- InformaciónDocument14 pagesInformaciónAlondraPas encore d'évaluation
- Thời gian làm bài: 60 phút: Kỳ Thi Học Kỳ I Năm Học 2017-2018Document40 pagesThời gian làm bài: 60 phút: Kỳ Thi Học Kỳ I Năm Học 2017-2018Quynh TrangPas encore d'évaluation
- The Two Faces of Cell Division: Mitosis MeiosisDocument5 pagesThe Two Faces of Cell Division: Mitosis MeiosisJamie MakrisPas encore d'évaluation
- BiopsiesDocument13 pagesBiopsiesSubbu ManiPas encore d'évaluation
- NCM116 - Metabolic - Endocrine DisordersDocument24 pagesNCM116 - Metabolic - Endocrine DisordersDan Hizon100% (1)
- Mammo MidtermsDocument23 pagesMammo MidtermsCherie lou PizaPas encore d'évaluation