Vous aimerez peut-être aussi
- Full Download Ebook PDF Introductory Econometrics A Modern Approach 7th Edition by Jeffrey PDFDocument42 pagesFull Download Ebook PDF Introductory Econometrics A Modern Approach 7th Edition by Jeffrey PDFtimothy.mees27497% (39)
- URBAN Tezis PDFDocument65 pagesURBAN Tezis PDFthieverPas encore d'évaluation
- Indications and Clinical Outcomes of High Tibial Osteotomy A Literature ReviewDocument8 pagesIndications and Clinical Outcomes of High Tibial Osteotomy A Literature ReviewPaul HartingPas encore d'évaluation
- Basic Surgical Principles With ITI ImplantsDocument10 pagesBasic Surgical Principles With ITI ImplantsEliza DN100% (1)
- Commissuroplasty: Sean M Parsel, DO, Ryan D Winters, MDDocument5 pagesCommissuroplasty: Sean M Parsel, DO, Ryan D Winters, MDAndy HongPas encore d'évaluation
- Piezoelectric Bone Surgery A New ParadigmDocument386 pagesPiezoelectric Bone Surgery A New ParadigmMihalache Catalin100% (1)
- MARTELINO Vs Alejandro DigestDocument1 pageMARTELINO Vs Alejandro Digestheirarchy100% (2)
- Secondary Fracture Prevention: An International PerspectiveD'EverandSecondary Fracture Prevention: An International PerspectiveMarkus J. SeibelPas encore d'évaluation
- Dr. Yoseph - The Role of Radiotherapy in The Management of Ameloblastoma and Ameloblastic CarcinomaDocument10 pagesDr. Yoseph - The Role of Radiotherapy in The Management of Ameloblastoma and Ameloblastic CarcinomaOnkologi Radiasi Angkatan 23Pas encore d'évaluation
- Ameloblastoma: Notorious Tumor of The Jaw - Report of A CaseDocument3 pagesAmeloblastoma: Notorious Tumor of The Jaw - Report of A CaseUwie MoumootPas encore d'évaluation
- The Occlusal Splint TherapyDocument5 pagesThe Occlusal Splint TherapyVíctor Adolfo Ravelo SalinasPas encore d'évaluation
- Radiographic Tumors PDFDocument58 pagesRadiographic Tumors PDFRiskha Febriani HapsariPas encore d'évaluation
- Dr. Lakshmi Narayana Malabar Cancer CentreDocument81 pagesDr. Lakshmi Narayana Malabar Cancer Centresherani999Pas encore d'évaluation
- Bisphosphonate Related Osteonecrosis of The Jaw (Bronj)Document33 pagesBisphosphonate Related Osteonecrosis of The Jaw (Bronj)jazzy penzPas encore d'évaluation
- Unicystic AmeloblastomaDocument5 pagesUnicystic AmeloblastomaayuPas encore d'évaluation
- Mucogingival ConditionsDocument2 pagesMucogingival ConditionsMuhammad Adel100% (1)
- Oral and Maxillofacial Surgery Cases: Emtenan Abdulrahmman Almajid, Alia Khalid AlfadhelDocument5 pagesOral and Maxillofacial Surgery Cases: Emtenan Abdulrahmman Almajid, Alia Khalid AlfadhelAmadea EmanuelaPas encore d'évaluation
- Dentigerous Cyst: A Retrospective Study of 20 Cases in S. S. Medical College Rewa, Madhya PradeshDocument4 pagesDentigerous Cyst: A Retrospective Study of 20 Cases in S. S. Medical College Rewa, Madhya PradeshnjmdrPas encore d'évaluation
- 16 - Fractures of The Zygomatic Complex and Arch - Pocket DentistryDocument22 pages16 - Fractures of The Zygomatic Complex and Arch - Pocket Dentistrydrgurpal74100% (1)
- TMJ DislocationDocument56 pagesTMJ DislocationAlok BhardwajPas encore d'évaluation
- Bitewing and Occlusal 2021Document47 pagesBitewing and Occlusal 2021Khadyjah RashidPas encore d'évaluation
- Fibrous Dysplasia PowerPoint PresentationDocument29 pagesFibrous Dysplasia PowerPoint PresentationAustinPas encore d'évaluation
- CBCT Third Eye in Dental ImplantDocument24 pagesCBCT Third Eye in Dental ImplantNajeeb Ullah100% (1)
- Benign Odontogenic Tumors of Jaws (AmeloblastomaDocument70 pagesBenign Odontogenic Tumors of Jaws (Ameloblastomagalina poberezhnikPas encore d'évaluation
- 1200 Walker MelissaDocument55 pages1200 Walker Melissazano_adamPas encore d'évaluation
- A Review of The Surgical Protocol For Reconstruction of Alveolar Ridge DeficiencyDocument21 pagesA Review of The Surgical Protocol For Reconstruction of Alveolar Ridge DeficiencyAymen Elatrash100% (1)
- Unicystic Ameloblastoma of The Mandible - An Unusual Case Report and Review of LiteratureDocument5 pagesUnicystic Ameloblastoma of The Mandible - An Unusual Case Report and Review of LiteratureChristian Ivan SantosoPas encore d'évaluation
- Maxillofacial Reconstruction 2013Document237 pagesMaxillofacial Reconstruction 2013Mohammed Qasim Al-WataryPas encore d'évaluation
- Molecular Etiopathogenesis of Ameloblastoma CurrentDocument5 pagesMolecular Etiopathogenesis of Ameloblastoma CurrentRiskha Febriani HapsariPas encore d'évaluation
- Principles of Tissue Biopsy in Oral and MaxillofacialDocument34 pagesPrinciples of Tissue Biopsy in Oral and MaxillofacialEdmond Apriza DrgPas encore d'évaluation
- Treatment of Long Term Anterior Dislocation of TMJDocument22 pagesTreatment of Long Term Anterior Dislocation of TMJXavir KhanPas encore d'évaluation
- Management of Pediatric Mandible Fractures PDFDocument16 pagesManagement of Pediatric Mandible Fractures PDFarfahPas encore d'évaluation
- 3205 All On Four Concept in Implant Dentistry A Literature ReviewDocument7 pages3205 All On Four Concept in Implant Dentistry A Literature ReviewAngelaBaleaPas encore d'évaluation
- Muscle Examination With Middle 3 Fingers With 1-2 Second ThrustsDocument4 pagesMuscle Examination With Middle 3 Fingers With 1-2 Second ThrustsFahad QiamPas encore d'évaluation
- Mandibular FracturesDocument171 pagesMandibular FracturesBalen ShalawPas encore d'évaluation
- Recent Advances in Diagnostic Oral MedicineDocument6 pagesRecent Advances in Diagnostic Oral Medicinegayathrireddy varikutiPas encore d'évaluation
- Premalignant Conditions of The Oral Cavity: Peter A. Brennan Tom Aldridge Raghav C. Dwivedi EditorsDocument285 pagesPremalignant Conditions of The Oral Cavity: Peter A. Brennan Tom Aldridge Raghav C. Dwivedi EditorsShantanu DixitPas encore d'évaluation
- Infectious Diseases of Oral CavityDocument21 pagesInfectious Diseases of Oral CavityhunarsandhuPas encore d'évaluation
- Desmoplastic Ameloblastoma of Anterior Mandible: Case Report of A RarityDocument5 pagesDesmoplastic Ameloblastoma of Anterior Mandible: Case Report of A RarityBimalKrishnaPas encore d'évaluation
- The Biological Bone AugmentationDocument70 pagesThe Biological Bone AugmentationSaman Mohammadzadeh100% (1)
- The Use of The Buccal Fat Pad Flap For Oral Reconstruction: Review Open AccessDocument9 pagesThe Use of The Buccal Fat Pad Flap For Oral Reconstruction: Review Open Accessmehak malhotraPas encore d'évaluation
- Aneurysmal Bone Cyst of The Zygomatic Arch Causing Limited Mouth OpeningDocument7 pagesAneurysmal Bone Cyst of The Zygomatic Arch Causing Limited Mouth OpeningAnonymous p28Tktgl5Pas encore d'évaluation
- The Biophysics of Mandibular Fractures - An Evolution Toward UnderstandingDocument13 pagesThe Biophysics of Mandibular Fractures - An Evolution Toward UnderstandingMikeunoePas encore d'évaluation
- Cysts of The JawsDocument75 pagesCysts of The JawsSwetha KaripineniPas encore d'évaluation
- Case Report Redy-Histologic Variants of AmeloblastomaDocument6 pagesCase Report Redy-Histologic Variants of Ameloblastomariris roselinaPas encore d'évaluation
- Erythema MultiformeDocument3 pagesErythema MultiformeLindar Rin リンPas encore d'évaluation
- Salivary Gland RadiologyDocument110 pagesSalivary Gland RadiologyHeba S RadaidehPas encore d'évaluation
- Rosa 2014Document6 pagesRosa 2014Michal PerkowskiPas encore d'évaluation
- Distraction OsteogenesisDocument28 pagesDistraction OsteogenesisManika SinghalPas encore d'évaluation
- Zygomatic Complex FracturesDocument128 pagesZygomatic Complex FracturesTarun KashyapPas encore d'évaluation
- Bicon Short Implant 2Document6 pagesBicon Short Implant 2Bicon Implant InaPas encore d'évaluation
- Distraction OsteogenesisDocument26 pagesDistraction OsteogenesissprapurPas encore d'évaluation
- Anatomy of Gingiva and Um - Pros Tho Don Tic SignificanceDocument108 pagesAnatomy of Gingiva and Um - Pros Tho Don Tic SignificanceDilip Singh100% (1)
- Surgical Treatment For Temporomandibular Joint Disorders ObjectivesDocument29 pagesSurgical Treatment For Temporomandibular Joint Disorders Objectivessergiusz9Pas encore d'évaluation
- Distraction Osteogenesis SeminarDocument126 pagesDistraction Osteogenesis SeminarkeerthanPas encore d'évaluation
- Bone Ring 3Document4 pagesBone Ring 3Pradusha RevuruPas encore d'évaluation
- Temporomandibular JointDocument86 pagesTemporomandibular Jointdrpankajaapaliya100% (2)
- Non-Odontogenic Tumor (Lecture)Document64 pagesNon-Odontogenic Tumor (Lecture)shabeelpn86% (7)
- Erythema Multiforme-Oral Variant: Case Report and Review of LiteratureDocument4 pagesErythema Multiforme-Oral Variant: Case Report and Review of LiteratureMarniati JohanPas encore d'évaluation
- Current Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderD'EverandCurrent Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderPas encore d'évaluation
- Craniofacial Disorders – Orofacial Features and Peculiarities in Dental TreatmentD'EverandCraniofacial Disorders – Orofacial Features and Peculiarities in Dental TreatmentÉvaluation : 2 sur 5 étoiles2/5 (1)
- Annex A - Scope of WorkDocument4 pagesAnnex A - Scope of Workمهيب سعيد الشميريPas encore d'évaluation
- 377 Situational Expression Advanced Level Test Quiz Online Exercise With Answers 1Document7 pages377 Situational Expression Advanced Level Test Quiz Online Exercise With Answers 1zdravkamajkicPas encore d'évaluation
- Beng (Hons) Telecommunications: Cohort: Btel/10B/Ft & Btel/09/FtDocument9 pagesBeng (Hons) Telecommunications: Cohort: Btel/10B/Ft & Btel/09/FtMarcelo BaptistaPas encore d'évaluation
- Chalcedony Value, Price, and Jewelry Information - International Gem SocietyDocument8 pagesChalcedony Value, Price, and Jewelry Information - International Gem Societyasset68Pas encore d'évaluation
- Family Factors: Its Effect On The Academic Performance of The Grade 6 Pupils of East Bayugan Central Elementary SchoolDocument11 pagesFamily Factors: Its Effect On The Academic Performance of The Grade 6 Pupils of East Bayugan Central Elementary SchoolGrace Joy AsorPas encore d'évaluation
- Case Study Managerial EconomicsDocument4 pagesCase Study Managerial EconomicsZaza Afiza100% (1)
- Sinamics g120p Cabinet Catalog d35 en 2018Document246 pagesSinamics g120p Cabinet Catalog d35 en 2018Edgar Lecona MPas encore d'évaluation
- 2022 NEDA Annual Report Pre PubDocument68 pages2022 NEDA Annual Report Pre PubfrancessantiagoPas encore d'évaluation
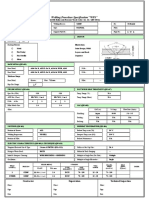
- Wps For Carbon Steel THK 7.11 GtawDocument1 pageWps For Carbon Steel THK 7.11 GtawAli MoosaviPas encore d'évaluation
- Portfolio Final AssignmentDocument2 pagesPortfolio Final Assignmentkaz7878Pas encore d'évaluation
- School Clinic Action PlanDocument2 pagesSchool Clinic Action PlanAlera Kim100% (7)
- Routine Maintenance For External Water Tank Pump and Circulation Pump On FID Tower and Rack 2017-014Document5 pagesRoutine Maintenance For External Water Tank Pump and Circulation Pump On FID Tower and Rack 2017-014CONVIERTE PDF JPG WORDPas encore d'évaluation
- Rate If Iodine and PropanoneDocument3 pagesRate If Iodine and Propanoneshareef1Pas encore d'évaluation
- GSE v. Dow - AppendixDocument192 pagesGSE v. Dow - AppendixEquality Case FilesPas encore d'évaluation
- DXFtoGerberConversionGuide Rev2!12!10 13Document8 pagesDXFtoGerberConversionGuide Rev2!12!10 13Tomasz BarwińskiPas encore d'évaluation
- Master Data FileDocument58 pagesMaster Data Fileinfo.glcom5161Pas encore d'évaluation
- Merging Shapes - 10 Minutes To Better Painting - Episode 1Document12 pagesMerging Shapes - 10 Minutes To Better Painting - Episode 1Nguyên HàPas encore d'évaluation
- Vertical Cutoff WallsDocument18 pagesVertical Cutoff WallsMark LaiPas encore d'évaluation
- Course Outline Cbmec StratmgtDocument2 pagesCourse Outline Cbmec StratmgtskyiePas encore d'évaluation
- 5000-5020 en PDFDocument10 pages5000-5020 en PDFRodrigo SandovalPas encore d'évaluation
- ISSA2013Ed CabinStores v100 Часть10Document2 pagesISSA2013Ed CabinStores v100 Часть10AlexanderPas encore d'évaluation
- Manual TV Hyundai HYLED3239iNTMDocument40 pagesManual TV Hyundai HYLED3239iNTMReinaldo TorresPas encore d'évaluation
- Ep Docx Sca SMSC - V2Document45 pagesEp Docx Sca SMSC - V290007Pas encore d'évaluation
- Net Pert: Cable QualifierDocument4 pagesNet Pert: Cable QualifierAndrés Felipe Fandiño MPas encore d'évaluation
- Bobcat E34 - E35Z Brochure - Adare MachineryDocument8 pagesBobcat E34 - E35Z Brochure - Adare MachineryNERDZONE TVPas encore d'évaluation
- Load Schedule: DescriptionDocument1 pageLoad Schedule: Descriptionkurt james alorroPas encore d'évaluation
- MPPSC ACF Test Paper 8 (26 - 06 - 2022)Document6 pagesMPPSC ACF Test Paper 8 (26 - 06 - 2022)Hari Harul VullangiPas encore d'évaluation
- Small Business and Entrepreneurship ProjectDocument38 pagesSmall Business and Entrepreneurship ProjectMădălina Elena FotachePas encore d'évaluation