Vous aimerez peut-être aussi
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Interfaith Peace VigilDocument2 pagesInterfaith Peace VigilRaphael McNamaraPas encore d'évaluation
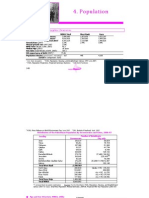
- Population: Topographic Features: Average Annual Rainfall Highest Elevation Lowest Elevation (1967-1998)Document3 pagesPopulation: Topographic Features: Average Annual Rainfall Highest Elevation Lowest Elevation (1967-1998)Raphael McNamaraPas encore d'évaluation
- Systematic & Institutionalised Ill-Treatment & Torture of Palestinian Children by IL AuthoritiesDocument118 pagesSystematic & Institutionalised Ill-Treatment & Torture of Palestinian Children by IL Authoritieszeitgeist-explorateurPas encore d'évaluation
- 5 RefugeesDocument2 pages5 RefugeesRaphael McNamaraPas encore d'évaluation
- The Gaza Strip 2007 Mediterranean SeaDocument1 pageThe Gaza Strip 2007 Mediterranean SeaRaphael McNamaraPas encore d'évaluation
- Targeted Civilians: A PCHR Report On The Israeli Military Offensive Against The Gaza Strip (27 December 2008 - 18 January 2009)Document184 pagesTargeted Civilians: A PCHR Report On The Israeli Military Offensive Against The Gaza Strip (27 December 2008 - 18 January 2009)Raphael McNamaraPas encore d'évaluation
- 2009 Without Trial: Administrative Detention of Palestinians by Israel and The Incarceration of Unlawful Combatants Law Joint Report, October 2009Document80 pages2009 Without Trial: Administrative Detention of Palestinians by Israel and The Incarceration of Unlawful Combatants Law Joint Report, October 2009Raphael McNamaraPas encore d'évaluation
- List Palestinian Civilians January 2009Document101 pagesList Palestinian Civilians January 2009levantepoente7073100% (2)
- Gaza Over and OverDocument70 pagesGaza Over and OverAlshaimaaPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Chapter Two Feasibility Study 2.0 Methods of Producing Ammonium Sulphate, ( (NH) SO)Document9 pagesChapter Two Feasibility Study 2.0 Methods of Producing Ammonium Sulphate, ( (NH) SO)Adeyoju RebeccaPas encore d'évaluation
- Mechanical Smoke Ventilation Calculations For Basement (Car Park)Document7 pagesMechanical Smoke Ventilation Calculations For Basement (Car Park)Mahmoud Abd El-KaderPas encore d'évaluation
- Chapter Eight - Vapour Compression CycleDocument37 pagesChapter Eight - Vapour Compression Cyclealhusseny100% (1)
- Harrington SOAP NoteDocument5 pagesHarrington SOAP NoteDanielle100% (4)
- Action Plan Gulayan Sa PaaralanDocument2 pagesAction Plan Gulayan Sa PaaralanAntonio ArienzaPas encore d'évaluation
- Module Letter 1Document2 pagesModule Letter 1eerolePas encore d'évaluation
- My Ideal Home: Name No. Class Date Mark TeacherDocument5 pagesMy Ideal Home: Name No. Class Date Mark TeacherQuadrado MágicoPas encore d'évaluation
- Heating and Cooling Load Calculations-ReportDocument20 pagesHeating and Cooling Load Calculations-ReportEhtisham Tanvir100% (1)
- CR300 Wireless Communication ProtocolDocument130 pagesCR300 Wireless Communication ProtocolHenry Martinez BedoyaPas encore d'évaluation
- Bosch Rexroth EFC3600 Manual PDFDocument238 pagesBosch Rexroth EFC3600 Manual PDFHomero Rios PeñaPas encore d'évaluation
- Critical Thinking and It's Importance in Education: I. Lenin Assistant Professor Auce KaraikudiDocument5 pagesCritical Thinking and It's Importance in Education: I. Lenin Assistant Professor Auce KaraikudiPABLO RAMIRO AGUILAR GONZALEZPas encore d'évaluation
- Bugreport Dandelion - Eea QP1A.190711.020 2022 02 15 07 45 54Document9 715 pagesBugreport Dandelion - Eea QP1A.190711.020 2022 02 15 07 45 54João Carlos Pereira ChoinasPas encore d'évaluation
- Asms 02 0033Document6 pagesAsms 02 0033Delfia AkiharyPas encore d'évaluation
- How To Make FireworksDocument14 pagesHow To Make FireworksLeonardo BiancoPas encore d'évaluation
- Aerody Design of BladeDocument90 pagesAerody Design of BladeB Bala Venkata GaneshPas encore d'évaluation
- Growth Rate and Fattening Potetial of Meat AnimalsDocument54 pagesGrowth Rate and Fattening Potetial of Meat AnimalsMuhammad Shahzad ChandiaPas encore d'évaluation
- Sawla - Laska (Lot - I) Road Project Hydrology - Hydraulics MDocument64 pagesSawla - Laska (Lot - I) Road Project Hydrology - Hydraulics Mashe zinab100% (2)
- Natural Topography of PakistanDocument25 pagesNatural Topography of Pakistansatayish100% (1)
- I10 Workshop Manual - ADocument292 pagesI10 Workshop Manual - ANorthstartechnology Company82% (11)
- Norma ASTM C171Document2 pagesNorma ASTM C171Jony Gutiérrez100% (1)
- Semicounductors & Pn-Junction (Complete)Document47 pagesSemicounductors & Pn-Junction (Complete)Khalid AliPas encore d'évaluation
- BF02692337 PDFDocument2 pagesBF02692337 PDFHitesh LokePas encore d'évaluation
- MEAMTA2-Assignment 2Document5 pagesMEAMTA2-Assignment 2pfukanisibuyi7Pas encore d'évaluation
- DHI-ITALE-060AA-P: White Strobe LampDocument2 pagesDHI-ITALE-060AA-P: White Strobe LampXlabs MedanPas encore d'évaluation
- Geo-Technical Investigation On Black Cotton Soils: GeotechnicalinvestigationonblackcottonsoilsDocument5 pagesGeo-Technical Investigation On Black Cotton Soils: GeotechnicalinvestigationonblackcottonsoilsDevendrasinh PadhiyarPas encore d'évaluation
- Experiment - 5Document26 pagesExperiment - 5Dilip GangopadhyayPas encore d'évaluation
- Preventive Pump SetDocument67 pagesPreventive Pump Setwtpstp sardPas encore d'évaluation
- Yamaha MG16 PDFDocument2 pagesYamaha MG16 PDFmiskoyu027Pas encore d'évaluation
- Hipertensiunea Arteriala - Cauze Si TratamenteDocument25 pagesHipertensiunea Arteriala - Cauze Si TratamenteClaudia MurguPas encore d'évaluation
- Ap2 Safe ManipulationDocument5 pagesAp2 Safe ManipulationDarthVader975Pas encore d'évaluation