Académique Documents
Professionnel Documents
Culture Documents
Book
Transféré par
wawa33850%(1)0% ont trouvé ce document utile (1 vote)
54 vues34 pagesBook
Copyright
© © All Rights Reserved
Formats disponibles
PDF, TXT ou lisez en ligne sur Scribd
Partager ce document
Partager ou intégrer le document
Avez-vous trouvé ce document utile ?
Ce contenu est-il inapproprié ?
Signaler ce documentBook
Droits d'auteur :
© All Rights Reserved
Formats disponibles
Téléchargez comme PDF, TXT ou lisez en ligne sur Scribd
0%(1)0% ont trouvé ce document utile (1 vote)
54 vues34 pagesBook
Transféré par
wawa3385Book
Droits d'auteur :
© All Rights Reserved
Formats disponibles
Téléchargez comme PDF, TXT ou lisez en ligne sur Scribd
Vous êtes sur la page 1sur 34
Introduction to Medical Ethics
Medical Ethics in the Global Village
Ray Noble
Centre for Reproductive Ethics and Rights
UCL Institute of Womens Health
London, UK
2
Introduction to Medical Ethics
Medical Ethics in the Global Village
Ray Noble
Centre for Reproductive Ethics and Rights
UCL Institute for Womens Health
London
A course in Medical Ethics at ASRAM, Andhra Pradesh, India
December 2007
Ray Noble 2007
All rights to the dissemination and distribution of the material in this booklet are reserved.
Supported by British Council UKIER Initiative
3
Contents
Aims and Objectives 4
Introduction to Medical Ethics 5
Practical Ethics 7
Human Rights and medical practice 13
Informed Consent 15
Keeping patients alive, well-being and futility 17
Case scenario 1: Autonomy and informed consent 18
Case scenario 2: Autonomy and Confidentiality 19
Case scenario 3 informing patients of bad news from a diagnosis 20
Case scenario 4 extremely premature babies, quality of life, sanctity of life 21
Case Scenario 5a refusal of treatment in pregnancy 22
Case Scenario 5b blood transfusion in neonatal intensive care 23
Case Scenario 6 Caesarean section patient choice 24
Scenario 7 fertility treatment and confidentiality 25
Scenario 8 - HIV in Pregnancy 26
Public health a consideration of utilitarian ethics 27
Clinical Research Ethics 29
Informed consent from minors - Gillick-competence 30
Hereditary disease and confidentiality 31
Conclusion 33
Answers to questions 34
4
Aims and Objectives
The aim of this course is to provide, through a series of workshops, an understanding of medical ethics and how
it is applied in clinical practice.
At the end of the course the student should be able to:
1) describe and discuss the principal strands of ethical thought
2) systematically apply them to ethical dilemmas in clinical practice and how they might best be dealt with
The student should gain an understanding of and be able to demonstrate in practice
1) Utilitarianism
2) Deontology
3) The Principles approach to medical ethics and how they are applied
4) Autonomy
5) Informed consent
6) Confidentiality
7) Human Rights as applied to medicine
The objective of each workshop is for students working in small groups to apply systematically key ethical
principles to specific case scenarios to provide a deeper understanding of the complexity of the ethical
dilemmas involved and to give practice in finding solutions to them. The overall aim is to increase awareness of
the complexity of ethical issues by addressing key examples in clinical practice so that students learn to
incorporate an ethical approach in medical practice.
DUTIES
UTILITY
PRINCIPLES
5
Introduction to Medical Ethics
What is Ethics? What does it do and how does it work?
Ethics is an understanding of the nature of conflicts arising from moral imperatives
1
and how best we may deal
with them. Specifically it deals with conflicts in potential outcome (consequences of actions) or with duties and
obligations. Ethics does NOT decide what is morally right or wrong; rather it considers how we should act best
in the light of our duties and obligations as moral agents. Clinicians have specific duties of care to their patients
and to society. It is generally held that clinicians should always act in the best interest of their patients; but
sometimes there is a conflict between obligations to a patient and those perceived to be owed to the community
or to other patients. It may not always be the case that what the clinician believes is in the best interest of the
patient is what the patient wishes or will consent to. Central to modern medical ethics is a respect for patient
autonomy
2
and the fundamental principle of informed consent.
Medical Ethics is a practical subject as well as a branch of moral philosophy.
Ethics is an integral part of good medical practice. It is an essential branch of medicine.
Ethics deals with the choices we make and our actions in relation to those choices. It deals with choices made
by both clinicians and patients and the duties and obligations of clinicians to their patients. Medical ethics also
deals with the choices made by society, the distribution of resources and access to health care and the dilemmas
arising from them.
Ethics deals with choices. Where there are no choices there is no need for ethics. There are almost always
choices to consider and there is almost always a need for ethics.
Any choice we make involves ethics, although sometimes we may not realise or consider it. How we live
involves choices affecting ourselves and others with both the potential for benefit and for harm (consequences)
3
.
How we feed ourselves, clothe ourselves, keep ourselves warm, travel to work etc. All these choices have
consequences for others.
Ethics is also about duties and obligations: to whom we have duties, how extensive they are, how best they may
be discharged and how we deal with conflicting duties and obligations
4
. Patients have duties and obligations
too, which is why we should respect them as moral agents. Parents have duties of care to their children; and
sometimes a clinicians duty to a child patient may conflict with those of the parents, and this needs an ethical
approach to resolve.
Ethical practice involves a systematic approach to decision making and actions, considering the interests of
all affected by the decision.
Remember: In those situations where you consider you have a duty to people other than your patient, a key
issue is how best you discharge these duties in the best interest of both parties. A duty of care is paramount in
the relationship between clinician and patient. For example, if a clinician must breech confidentiality of a
1
A moral imperative is one determined by duty. A categorical imperative is one which is not dependent on outcome or
restricted by reservations; it is simply determined by duty.
2
Patients are also moral agents with the capacity to decide what is in their best interests if they are appropriately informed.
3
Utilitarian ethics considers justification of decisions in relation to outcome benefits and harms.
4
Deontological ethics considers justification of decisions in relation to duties and obligations. Deontology simply means the
study of duty.
6
patient, they should consider not only whether they should do so
5
, but also how they should do so in the best
interest of their patient.
5
There must be very specific circumstances for this to apply. Confidentiality is a key factor in the trust between clinician and
patient.
7
Practical Ethics
In practical ethics we apply a systematic approach. In general we apply four major ethical considerations.
First, we must define the nature of the problem. What is the major ethical dilemma? We need a clear
understanding of the nature of the dilemma or dilemmas.
Consider this example:
A baby born prematurely at 24 weeks gestation is put in intensive care. However she is not thriving and
scans suggest she has profound brain damage. She cannot breathe unassisted and the care team believe
she is suffering and it is not in her interest to keep her alive. The parents do not agree. What should the
clinician do?
We can usually dissect problems by considering
1) Consequences: what are the consequences of any given course of action?
Consider both benefits and harms
2) Duties and Obligations: what are the duties of the clinician? Does the dilemma arise from a conflict
of duties? To whom does the clinician owe these duties? If so how best can this dilemma be
resolved?
3) Consider the categorical imperatives. For example, is it a case of respect for autonomy or informed
consent?
4) Application of principles. How might the four key principles of ethical clinical practice (see below)
be applied?
Ethics is NOT a set of rules, nor is it a formula: following rules blindly or rigidly is likely to lead to
unethical practice because it fails to take account of circumstances or specific exceptions and fails to
recognise new dimensions. Each case should be treated on its merits and specific circumstances (for
example not all premature babies will have the same outcome). A one rule fits all approach might be
unethical as it fails to consider the specific interests of those involved.
Ethics DOES seek to set up guidelines to act as signposts to good ethical practice. Always consider any
guidelines issued by medical professional bodies; but be prepared for exceptions. Also, guidelines may
change in the light of experience and new evidence. Keep yourself informed of any changes in
guidelines.
Ethics is a complex tapestry, a picture with many colours and strands.
There are two primary strands of thought:
1. Utilitarian considers the balance of benefits and harms were outcome may justify the action
(ends justify means)
2. Deontological considers duties and obligations and how best they may be met. Outcome may
not be sufficient to justify action (ends alone may not justify means).
8
The utilitarian approach
6
is attractive because it appears to provide an empirical solution to ethical
dilemmas. If we can assess potential benefits and harms they can be weighed, and a balanced judgment
made on the proportionate good achieved by a given action or choice. The greater the amounts of benefit
for a given amount of potential or actual harm then the more likely it is that the action can be justified.
Put another way, the greater the amount of potential harm for a given benefit the less likely it is that the
action can be justified. The problem then is to determine 1) the necessary ratio of benefit to harm and 2)
how these are measured and weighed and 3) who should make the choice. A specific problem occurs
when a group for whom there is a risk of harm is not the group likely to receive any benefit, as is often
the case in clinical research trials. An example of the utilitarian approach is the consideration applied to
resuscitation and keeping very premature babies in intensive care: for any given case a pragmatic
judgment may be made on the likely benefits and harms. General policy on these babies is determined
by the proportions of such babies demonstrated to have profound morbidity
7
- i.e. an evidence-based
assessment. In practice however the ethical problems are much more complex, involving issues about
who makes the decision, informed consent, the right to life and other such considerations factors
which are not subject to empirical solutions.
In contrast, duties and obligations are rarely determined by empirical data they are difficult to
quantify or measure and they are extremely difficult to partition it would, for example, be very
difficult to understand a concept of half a duty. Nevertheless, medical ethics in practice is in large part a
consideration of duties and conflicts of duty. The ethical consideration here is focused on who has the
duty; to whom it is owed, how extensive it is and how best it can be discharged. The onus of a duty and
how it is discharged depends on an ability to discharge it. Whilst the onus of duty exists independent of
outcome, it might be possible to resolve a conflict of duty by considering implications of any given
decision in the discharge of those duties. Consider a person who has been asked to look after a dog
whilst also caring for children playing on playground swings and roundabouts. How best should this
person discharge their duty if the dog should run off? Consider a family practitioner who is treating a
patient for a sexually transmitted disease and this patients partner is also one of the GPs patients.
The distinction between the utilitarian (or consequentialist
8
) and the deontology approaches is made
clearer by considering the following:
When considering the choice between two alternative actions, A and B, the consequentialist approach
considers which of the two choices is likely to produce the greatest net benefit. Consider, however, what
should happen if B is likely to produce the most benefit but A has been promised.
There are several ways to consider this problem. A strictly consequentialist view might consider the
result of breaking the promise in the net evaluation of benefits and harms, adhering to the view that the
ends might still justify the means (including breaking the promise) if the net benefit is sufficient to
outweigh the cost of breaking the promise (such costs may involve considerations such as loss of trust
and unhappiness at the decision). In the consequentialist approach, the making or breaking of promises
6
Quinton, A. Utilitarian Ethics. (2
nd
Edition 1989) Duckworth. London, UK.
7
Some countries have adopted a cut off at a given gestational age. In Holland for example the cut off is at 26 weeks; babies
below this gestational age are not resuscitated. In the UK a pragmatic decision is made by clinicians on a case by case basis.
8
Not all consequentialist systems are strictly utilitarian; what they have in common is that actions may be justified by
outcome. What are considered as good outcomes may differ between systems.
9
is simply viewed as part of the actions and outcomes; they hold no inherent value
9
. The deontological
approach considers the promise as a duty, the breech of which requires specific justification involving a
conflict of duties (say the duty to keep the promise against the duty to do what is in the best interest of
the patient, or community). This emphasis on outcome on the one hand and duty on the other may lead
to different resolutions.
The Principles approach.
Four fundamental principles are often applied in modern medical ethics
10
:
1. Respect for individual autonomy individuals are regarded as moral agents with duties and
obligations and the capacity to understand and make ethical decisions.
2. Principle of beneficence seek to do good
3. Principle of non-maleficence avoid doing harm
4. Principle of Justice people should be treated fairly.
However, applying any one of these principles may sometimes conflict with one or more of the others.
For example, applying principles 2 and 3 in relation to a mentally ill patient may conflict with 1 and
possibly 2. Can you think of other specific examples?
Consider these principles in relation to the case of the premature baby presented above. How should the
clinician resolve principles 2 and 3? Where do the parents stand in relation to principle 1?
Paternalism doctor knows best the exception not the rule
Modern medicine seeks to avoid a paternalistic (doctor knows best) approach to their patients. Instead it
considers the doctor and patient mutually engaging in the decision making with the final decision on
treatment options being that of the patient. Respect for autonomy, informed consent and
confidentiality are now key markers for ethical practice and there must be exceptional circumstances or
reasons for breeching them.
Nevertheless, there may be circumstances where the paternalistic approach is still a major factor.
Consider again the case of the profoundly sick premature baby in intensive care presented above. A key
approach here for ethical practice is to consider how best the clinician should act in the interest of this
baby whilst still respecting the involvement of the parents in the decision.
Categorical
11
Imperative
12
It is useful to consider two kinds of motivation for ethical action. First there are those actions that are
justified or motivated by outcome. We can say that these are contingent or dependent on the
objective (what they seek to achieve, for example a greater good). The second type of action is special in
9
From a utilitarian perspective, promises would be considered to have value if in general they increase benefit to the greatest
number; thus promises have extrinsic value. Keeping promises has value in building trust; the confidence that in general
promises will be kept; else promises would have no value at all.
10
Beauchamp, T.L and Childress, J.F. Principles of biomedical ethics (5
th
Edition, 2001).
11
Categorical means: leaving no room for doubt, question, or contradiction
12
Imperative: absolutely necessary or unavoidable
10
that they are not justified or motivated by outcome or objective. Such actions are non-contingent, and
are both ethically means and ends in themselves (they are the greater good). For this reason they are also
said to be categorical.
When we consider categorical imperatives in ethics we are usually asking if there can be any exceptions
and what criteria should be applied to justify these exceptions.
13
Examples of categorical imperatives in modern medical ethics are respect for autonomy, informed
consent and confidentiality. Much of modern medical ethics is concerned with dilemmas arising from
these imperatives. Because they are categorical in nature, they set the ethical threshold very high
indeed.
Consider in what circumstances a clinician could or should act without the express consent of the patient
or the consent of someone acting on behalf of the patient (a relative for example); how the clinician
should proceed in such circumstances; in what circumstances could or should a clinician inform others
about their patients and how should they act in the best interests of their patient if such a breech in
confidentiality is necessary.
It has generally been held that respect for the sanctity of life is a categorical imperative of medical
ethics. Does this mean a clinicians duty is always to sustain life? Or are there some circumstances when
a respect for human dignity (another categorical imperative) requires the clinician to stop seeking to
sustain life and move to palliative care
14
to avoid the suffering of their patient? Practical ethics is
concerned with the guidelines for these choices and how they are best applied.
A key aspect to note here is that ethics is necessary because our categorical imperatives may often
conflict (a clash of fundamental principles). Ethics seeks to understand the nature of this problem and,
with practical ethics, how best we should proceed.
Which of the following do you consider to be the best description (hint: only one should be picked)?
1) Ethics decides what is right or wrong
2) Ethics decides what is moral
3) Ethics considers the nature of, and how best to deal with conflicts in moral imperatives
Which of the following is true (only one is true)?
1) Deontology is the consideration of duties and obligations
2) Deontology considers the balance of benefits and harms
3) Deontology considers that ends may justify means
Which of the following is true (more than one may be true)?
1. A Utilitarian approach in ethics considers the consequences of actions or choices
13
This appears contradictory because a categorical imperative by definition should have no exceptions. However, I find this a
useful approach because it means that the ethical threshold for any breech of these imperatives must be set extremely high
and the justification must be very special indeed. We might also say that such a justification must involve another, conflicting
moral imperative.
14
alleviating pain and symptoms without eliminating the cause
11
2. A Utilitarian approach in ethics considers that ends may justify means
3. A Utilitarian approach in ethics considers whether clinicians have discharged their duties in the
best interests of their patients.
Answers are discussed at the end of this booklet.
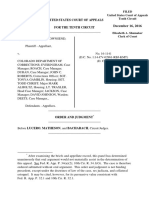
Two approaches to ethical analysis are shown in the diagram: in system B the ethics of an action are
determined by the balance of consequences benefits and harms (consequentialist system); in system A
the ethics is determined by reference to a measure which is independent of the outcome (an example of
this kind of system is the deontological approach considering duties and obligations).
In system B there is no concept of an inherent Good Good is simply the better outcome in terms of the
greatest increase in happiness or well-being.
In system A the concept of Good has an inherent moral value it is good for its own sake. In this
system, fulfilling a duty would be considered inherently good a good in itself.
The approach of this course and book emphasises that the two types of systems are not totally separate.
We may, for example, consider it a duty in general to act in a way which tends to increase well-being.
Nonetheless, they are fundamentally different in concept and application. Whether such a duty is
discharged sufficiently may be judged by the potential or predicted outcome. However, the fundamental
difference remains: the action is performed to fulfil the duty, and this may not necessarily be fulfilled by
producing the greatest possible increase in benefit.
The duty may require a different balance from that determined by utilitarian criteria alone (consider
again the example of the choice between alternatives A and B, where A produces the greatest overall net
benefit but B has been promised). The promise could just as readily be confidentiality, informed consent
or respect for patient autonomy. It is the nature of categorical imperatives that they cannot easily be
GOOD
ACTION
CONSEQUENCES
BENEFITS - HARMS
A B
12
bargained away. They increase the ethical threshold to a very high level. They require exceptional
circumstances before they can be breeched ethically, and in such circumstances we are usually dealing
with conflicting imperatives.
13
Human Rights and medical practice
We hold these truths to be self evident, that all men are created equal. American declaration of
independence, 1776. This statement of rights has sounded through to the modern day United Nations
Universal Charter of Human Rights adopted by the General Assembly in 1948:
All human beings are born free and equal in dignity and rights. They are endowed with reason and
conscience and should act towards one another in a spirit of brotherhood.
15
Before reading on consider which of these you consider to be the best ethical statement. Consider your
reasons for doing so.
All humans should be treated equally
All humans should be treated fairly
All humans should be given an equal consideration of their interests
Treating people equally in all circumstances would lead to unfairness because it would fail to take
account of differing physical and mental abilities or of the social and economic circumstances of the
individual. Treating people equally without regard for their interests, their abilities or their
circumstances is likely to be unfair.
Clearly from a moral sense (moral equality) we do not mean the same, or equal in terms of
endowment.
It is in the nature of the concept of moral equality that it is without measure. It is simply sufficient to be
human to command the respect in dignity and rights. If we had a measure of equality, then some humans
may not measure up. I cannot run a hundred metres in 10 seconds, nor am I an accomplished concert
pianist. From a moral perspective, however, I do expect to be given an equal consideration of my
interests and needs when I consult a medical practitioner. I certainly would not wish that they consider
my life to be of less value because I do not have these abilities. Central to the concept of human rights is
that they apply simply because someone is human and for no other reason.
Human rights are not a passive process. They are an active process requiring positive action. For
example in ethical medical practice the clinician should not simply obtain consent for procedures but
make every effort to be certain that the patient understands the consent i.e. that it is informed
consent. Sometimes this may not be possible for example where a patient is mentally incapacitated
such that it would be impossible for them to fully comprehend the relevant information. However, in
such circumstances their should be every effort to obtain consent from someone who might be their
guardian or who has a duty of care for them as, for example, a close relative; nor should language
difficulties be a barrier to obtaining fully informed consent.
15
Article 1. UN Universal Declaration of Human Rights (1948)
14
There has been much effort in recent decades to build the notion of human rights into medicine. For
example, an International Bioethics Committee was established in 1993 by UNESCO to consider the
impact of developments in biomedicine on human rights.
Human Rights provide a universal framework for ethical medical practice. It is debatable whether this
framework provides clear solutions to ethical dilemmas. It can be said to present a frame of moral
imperatives in the form of rights. As with all such imperatives they are as likely to throw up or expose
moral dilemmas as they are to solve them. Perhaps the major impact is in relation to discrimination and
justice, access to health care and empowerment.
Consider the following case scenario in relation to human rights:
A 16 year old girl is accompanied to a clinic by her parents. The girl has a low IQ (below 80). She is
pregnant and is having the pregnancy terminated. Her parents have requested that she also be sterilised
by tubal ligation
16
which they feel would be in her best interests as she is promiscuous and is not able to
understand contraceptive methods.
Should the clinician agree to this request? How should the clinician best deal with the request?
Human Rights - a Trump Card?
Human rights are often presented as though they are an ethical trump card. However, rather than
resolving issues, the application of human rights can just as readily create or reveal ethical problems.
Consider for example the concepts of a right to life and the right to be treated with dignity. An ethical
approach to clinical practice must often reconcile these two fundamentals. Consider for example the
decision to move from treatment to combat disease and preservation of life to a palliative regime
designed to minimise pain and suffering whilst allowing the disease to take its course. Such treatment
may also involve drugs that whilst minimising pain also hasten death.
This move to palliative care and ceasing to preserve a life is crucially different to active euthanasia the
aim of which is to end a life considered not worth living. Whilst the palliative treatment may hasten
death, this is a consequence of the treatment given to relieve pain and suffering, rather than the specific
objective of ending life. Arguably, it is not the result of a judgment that any given life is not worth
preserving. The difference ethically (and legally) is one of intention.
This is much more difficult when the suffering is psychological or where an existence is so restrictive or
involves handicap which whilst not necessarily producing physical pain nevertheless involves
substantial loss of dignity. Consider for example a patient with advanced Alzheimers disease or severe
motor neurone disease. From a human rights perspective we are dealing with the right to self-
determination. If such patients have expressed a wish not to have their lives preserved in such cases,
what then is the duty of the clinician? These concepts of human rights are allied to the categorical
imperatives considered elsewhere in this booklet. The right to self-determination would of necessity
incorporate not only informed consent but also informed refusal of treatment. In ethical practice there
must be consideration not solely of whether a clinician respects a patients wishes; of equal importance
is how the clinician does so.
16
Tubal Ligation is considered to be permanent in most circumstances. Reversal is difficult and expensive and is often than
unsuccessful.
15
Informed Consent
Informed consent is a key factor in modern ethical medical practice and great emphasis is placed upon it. The
main issue is not simply that consent to a procedure is obtained, but more importantly, how it is obtained; not
simply that the patients have been told of what happens in the procedure and what the key risks may be, but
how they are informed.
A patient should not be exposed to risk of harm unless he has agreed to that risk, which he/she cannot do
without being properly informed. This is particularly important where there are choices of treatment, each
carrying different types and levels of risk and potential outcomes. The circumstance of each patient will be
different and they may wish to make different choices about their health and lives. A terminally ill patient, for
example, may prefer a therapy which gives him a reasonable quality of life for a few months to be with his
family, than a drug regime that may prolong his life for longer but may involve a greater burden of sickness.
Clearly this is a personal decision, not solely a clinical one, and only the patient is in a position to decide which
option is best for him/her. But the patient cannot do so unless they are properly informed.
There are essentially two views of consent:
1. The first is a clinician-centred view, which is a legalistic approach to consent and considers what the
clinician should tell a patient about the nature of a procedure and the risks. It is the minimum required to
protect the clinician from a charge of common assault.
2. The second is a patient-centred view, which considers what is necessary to enable the patient to make an
informed choice. This is what is referred to in ethics as informed consent.
It is not always clear what information is necessary for informed consent. Informed consent is essentially an
enabling process. A judgment has to be made about what information is relevant and/or significant in enabling a
patient to make a reasonable choice that is appropriate for his/her circumstances. Informed consent is patient-
specific.
It does not mean that the patient should be informed of every conceivable risk no matter how small.
Informed consent requires that everything is done to ensure that the patient understands
1. The nature of the procedure what is to be done and in simple terms how it is to be done.
2. The risks involved (but as above, this is not simply a list of all possible risks). They are the most likely risks
and any that the patient themselves might be concerned about in making a decision. If a patient asks about a
risk that the clinician has not mentioned, then the clinician should inform the patient about that risk.
3. The consequences what are the likely outcomes of the procedure and alternatives
4. The alternatives this includes information about what the likely outcome would be if the patient chooses
not to have the procedure and any other alternative the patient themselves may ask about where relevant.
Informed consent is a matter of judgement. The key aspect is that it should be enabling for the patient. Ask not
what the clinician needs to tell the patient, but what the patient needs to know in order to make a reasonable
decision in the light of their needs and interests. A standard way to approach this is to ask what a reasonable
person would expect to be told in order to make an informed choice.
It is perfectly legitimate for a clinician to withhold information which they may believe to be unnecessarily
distressing (a therapeutic decision), but if such information is necessary for the patient to make a reasoned
16
decision then it should not be withheld. In such circumstances the clinician should consider how best such
information is given and in what circumstances for example, does it require further support or counselling;
should the patient have someone with them to support them etc. Patients respond to bad information in a
variety of different ways.
17
Keeping patients alive, well-being and futility
Consider the following case scenario:
A 12 year old child has undergone several treatment regimes for cancer over a period of years none of which
have been successful. New treatments might offer some benefit but are considered unlikely to lead to a
complete cure. Research trials indicate that the benefit can be between a few months to a year of life. After
much discussion the parents withhold their consent when the new treatment is suggested by the clinical
specialists at the hospital. The parents are concerned that the potential side effects outweigh the possible
extension of the childs life. They believe their child has already suffered enough over the years of treatment.
Consider what the clinicians should do and what factors should be taken into account.
Now consider the following similar case:
A 12 year old child has undergone several treatment regimes for cancer over a period of years none of which
have been successful. The parents have heard of a new treatment which clinical trials suggest might prolong life
of some cancer patients by between a few months and a year. As a result they have requested that this treatment
be given to their child. However, the specialist clinicians at the hospital do not believe there would be any
significant benefit for the child and that the side-effects of the treatment can often be debilitating.
Consider what the clinicians should do and what factors should be taken into account.
In what ways do the two scenarios differ? Do these differences lead to a different ethical approach?
Identify and consider the major ethical dilemmas apparent in these cases. Do they present more than one
dilemma?
Many cases will present with more than one major ethical dilemma.
18
Case scenario 1: Autonomy and informed consent.
Downs screening test: A pregnant woman decides to have a triple marker test for Downs screening.
After she has given the blood she decides she does not want to know the result as she wants to have the
baby. The test result shows a high risk of Downs syndrome. The clinician feels there will be a high
social and economic burden on the family and would like to convey the test result to the patient to
inform her decision making. What should the obstetrician do?
Apply the four major ethical considerations systematically.
What are the major ethical dilemmas?
1. Consequences: what are the consequences of any given course of action?
Consider both benefits and harms
2. Duties and Obligations: what are the duties of the clinician? Is this a case of conflict of duties?
To whom does the clinician owe these duties? If so how best can this dilemma be resolved?
3. Consider the categorical imperatives. Is this a case of respect for autonomy and informed
consent? If so are there sufficient grounds to ignore her wishes?
4. Application of principles. How might the four key ethical principles of ethical clinical practice
be applied?
What other considerations might apply?
What are your conclusions about the best course of action? Give your reasons.
What might be the reasons for the womans decision? Do you think a clinician is always best placed to
understand and judge these reasons?
Remember in ethics we cannot always provide a satisfactory resolution to all perceived problems.
Ethically there is a great deal that the clinician should consider in discharging his/her duty of care. If you
decide that the clinician should respect the womans wishes and not reveal the test result, is there
anything else the clinician should do in the discharge of his/her duty of care? Remember that the
clinician should ideally be a member of a care team.
19
Case scenario 2: Autonomy and Confidentiality
You are a doctor working in a busy practice in London, UK. One of your patients is a fifteen year old
girl who has come to see you to ask advice about contraception and sexually transmitted diseases. She
explains that she has a regular boyfriend with whom she is now having sexual intercourse. At age fifteen
in the UK she is considered a minor.
Apply the four major ethical considerations systematically.
What are the major ethical dilemmas?
1. Consequences: what are the consequences of any given course of action?
Consider both benefits and harms.
2. Duties and Obligations: what are the duties of the clinician? Is this a case of conflict of duties?
To whom does the clinician owe these duties? If so how best can this dilemma be resolved?
3. Consider the categorical imperatives. Is this a case of respect for autonomy and informed
consent? If so are there sufficient grounds to ignore her wishes?
4. Application of principles. How might the four key ethical principles of ethical clinical practice
be applied?
What other considerations might apply?
What are your conclusions about the best course of action? Give your reasons.
Do you think this is a case where one rule fits all? Or do you think each of such cases should be treated
according to circumstances? For example: would you take the girls level of comprehension and/or
maturity into account?
Remember in ethics we cannot always provide a satisfactory resolution to all perceived problems.
Ethically there is a great deal that the clinician should consider in discharging his/her duty of care. If you
decide that the clinician should respect the girls autonomy and not inform her parents, is there anything
else the clinician should do in the discharge of his/her duty of care? Ethics considers also how best to
make decisions and act upon them in the interest of patients. If you decide to inform her parents consider
how you should act best to discharge your duty to this young girl.
When you have finished considering this scenario read through the section on Informed consent from
minors on page x .
20
Case scenario 3 informing patients of bad news from a diagnosis
A 16 year old girl is referred with primary amenorrhea. Primary amenorrhea is usually caused by genetic
or congenital disorders and is often associated with developmental problems during puberty. In this case
no uterus can be found on a scan. Should the doctors inform the parents of the diagnosis before the
patient is informed, or should they inform the patient directly? How best should they proceed?
Apply the four major ethical considerations systematically.
What are the major ethical dilemmas?
1. Consequences: what are the consequences of any given course of action?
Consider both benefits and harms.
2. Duties and Obligations: what are the duties of the clinician? Is this a case of conflict of duties?
To whom does the clinician owe these duties? If so how best can this dilemma be resolved?
3. Consider the categorical imperatives. Is this a case of respect for autonomy and informed
consent?
4. Application of principles. How might the four key ethical principles of ethical clinical practice
be applied?
What other considerations might apply?
What are your conclusions about the best course of action? Give your reasons.
Do you think this is a case where one rule fits all? Or do you think each of such cases should be treated
according to circumstances? For example: would you take the girls level of comprehension and/or
maturity into account? Would you take her emotional state into account?
Remember in ethics we cannot always provide a satisfactory resolution to all perceived problems.
Ethically there is a great deal that the clinician should consider in discharging his/her duty of care. If you
decide that the clinician should respect the girls autonomy and not inform her parents first, is there
anything else the clinician should do in the discharge of his/her duty of care?
Consider how you might act if the parents are not available and the girl is asking for information.
Ethics considers also how best to make decisions and act upon them in the interest of patients. If you
decide to inform her parents first consider how you should act best to discharge your duty to this young
girl.
21
Case scenario 4 extremely premature babies, quality of life, sanctity of life.
A baby born prematurely at 23 weeks gestation is being kept in intensive care. However she is not
thriving and scans suggest she has profound brain damage. She cannot breathe unassisted and the
parents believe she is suffering and also that the quality of life she can expect will be very poor and
further treatment is harmful. The parents believe that her survival should be placed in the hands of God
and ask that the ventilator should be switched off. What should the clinicians do?
Apply the four major ethical considerations systematically.
What are the major ethical dilemmas?
1. Consequences: what are the consequences of any given course of action?
Consider both benefits and harms.
2. Duties and Obligations: what are the duties of the clinician? Is this a case of conflict of duties?
To whom does the clinician owe these duties? If so how best can this dilemma be resolved?
3. Consider the categorical imperatives. Is this a case of respect for autonomy and informed
consent? If so are there sufficient grounds to ignore her wishes?
4. Application of principles. How might the four key ethical principles of ethical clinical practice
be applied? If necessary remind yourself of these principles.
What other considerations might apply?
What are your conclusions about the best course of action? Give your reasons.
Do you think this is a case where one rule fits all
17
? Or do you think each of such cases should be
treated according to circumstances? If so who should make the final decision, particularly where parents
and clinicians are in disagreement about the benefits of keeping the baby alive?
17
In many countries such as in the UK the value of keeping very premature babies on life support is a balanced judgement
made on a case-by-case basis. In some countries such as Holland this has been determined with a general rule that no baby
born under 25 weeks gestation will be resuscitated and kept on intensive care.
22
Case Scenario 5a refusal of treatment in pregnancy.
You are a clinician working in a fetal medicine unit in a major city in the USA. The fetus of one of your
patients is likely to die unless a blood transfusion is given to replace fetal red blood cells that are being
destroyed by the Rh-sensitized mother's immune system. This treatment is meant to keep the fetus
healthy until he or she is mature enough to be delivered, but the woman refuses to give her consent to
this procedure for religious reasons (She is a Jehovahs Witness for whom blood transfusions are
forbidden). What should you do?
Apply the four major ethical considerations systematically.
What are the major ethical dilemmas?
1. Consequences: what are the consequences of any given course of action?
Consider both benefits and harms.
2. Duties and Obligations: what are the duties of the clinician? Is this a case of conflict of duties?
To whom does the clinician owe these duties? If so how best can this dilemma be resolved?
3. Consider the categorical imperatives. Is this a case of respect for autonomy and informed
consent? If so are there sufficient grounds to ignore her wishes?
4. Application of principles. How might the four key ethical principles of ethical clinical practice
be applied?
What other considerations might apply?
What are your conclusions about the best course of action? Give your reasons.
23
Case Scenario 5b blood transfusion in neonatal intensive care.
A very sick premature baby in intensive care must have blood samples taken regularly to check pH,
blood gases etc. The blood samples taken over time must be replaced or the baby will become anaemic
and is likely to die. The parents are Jehovahs Witnesses and refuse to give consent to this procedure
because it involves blood transfusion. What should the clinician do?
Apply the four major ethical considerations systematically.
What are the major ethical dilemmas?
1. Consequences: what are the consequences of any given course of action?
Consider both benefits and harms.
2. Duties and Obligations: what are the duties of the clinician? Is this a case of conflict of duties?
To whom does the clinician owe these duties? If so how best can this dilemma be resolved?
3. Consider the categorical imperatives. Is this a case of respect for autonomy and informed
consent? If so are there sufficient grounds to ignore her wishes?
4. Application of principles. How might the four key ethical principles of ethical clinical practice
be applied?
What other considerations might apply?
What are your conclusions about the best course of action? Give your reasons.
What are the key factors that are different in this case compared to Scenario 5a?
24
Case Scenario 6 Caesarean section patient choice
A pregnant woman with a previous section has been advised to go for a normal delivery for her 2
nd
delivery. While in labour, she wants to have a section because she is worried about a rupture of the
uterine scar. The clinicians are confident that the labour would progress without a complication. Should
the obstetrician do a section to abide by the patients wish?
Apply the four major ethical considerations systematically.
What are the major ethical dilemmas?
1. Consequences: what are the consequences of any given course of action?
Consider both benefits and harms.
2. Duties and Obligations: what are the duties of the clinician? Is this a case of conflict of duties?
To whom does the clinician owe these duties? If so how best can this dilemma be resolved?
3. Consider the categorical imperatives. Is this a case of respect for autonomy and informed
consent? If so are there sufficient grounds to ignore her wishes?
4. Application of principles. How might the four key ethical principles of ethical clinical practice
be applied?
What other considerations might apply?
Is this a case where a paternalistic approach is justified? Notwithstanding the confidence of the
obstetrician, are her anxieties reasonable in the light of risk of rupture?
What are your conclusions about the best course of action? Give your reasons.
One way to view this case is to consider the patient wishes in relation to consent to treatment. In other
cases clinicians might be suggesting a section and the pregnant woman refuses to give her consent to
this because she wants to have a natural birth. Also consider this in relation to the principle of non-
maleficence (doing no harm). If a clinician believes that a procedure is not in the best interests of the
patient, should he/she refuse to carry this out.
This dilemma is likely to become more common as many patients are more aware of possible alternative
treatments particularly as they can access information readily on the internet.
25
Scenario 7 fertility treatment and confidentiality.
A couple who have been married for ten years visit a gynaecologist for infertility treatment. The woman
has a history of irregular menstrual cycles. The Gynaecologist treats the patient to stimulate the ovaries
without success. After a few cycles of treatment the patient decides to see the gynaecologist on her own.
She reveals that she had never had cycles (primary amenorrhea). The patient does not wish her clinical
condition to be discussed with her husband because she is concerned about the consequences in relation
to her marriage. Considering that the doctor was consulted by the couple for fertility treatment, what
should the doctor do?
Apply the four major ethical considerations systematically.
What are the major ethical dilemmas?
1. Consequences: what are the consequences of any given course of action?
Consider both benefits and harms.
2. Duties and Obligations: what are the duties of the clinician? Is this a case of conflict of duties?
To whom does the clinician owe these duties? If so how best can this dilemma be resolved?
3. Consider the categorical imperatives. Is this a case of respect for autonomy and confidentiality?
If so are there sufficient grounds to ignore her wishes?
4. Application of principles. How might the four key ethical principles of ethical clinical practice
be applied?
What other considerations might apply?
What are your conclusions about the best course of action? Give your reasons.
26
Scenario 8 - HIV in Pregnancy
Antenatal screening for HIV has clear advantages:
A negative result can be reassuring, but if the result is positive, in the right circumstances of available
facilities and therapy:
The infection may be managed effectively
The woman can make an informed choice whether or not to continue with the pregnancy
The risk of maternal-child transmission can be reduced greatly
The woman can make an informed choice about her future fertility
The womans partner can also be tested and advice about contraceptive protection can be given
Consider the following options of strategy for HIV antenatal screening:
1. there should be compulsory antenatal screening for HIV
2. antenatal screening should be offered to all women but only carried out with their express
consent (an opt in strategy)
3. antenatal screening should be part of routine screening in pregnancy unless the woman
specifically requests that HIV screening should not be carried out (an opt out strategy)
In the UK, before 1999 an opt in strategy was applied. Antenatal screening for HIV was only carried
out with the express informed consent of the pregnant woman. From 1999 this changed to an opt out
strategy, and screening was carried out routinely unless the woman specifically requested that it should
not be done. As a result HIV status was picked up in many more women and with careful management
and antiretroviral therapy maternal-offspring transmission was reduced substantially.
Apply the four major ethical considerations systematically.
What are the major ethical dilemmas?
1. Consequences: what are the consequences of any given course of action?
Consider both benefits and harms.
2. Duties and Obligations: what are the duties of the clinician? Is this a case of conflict of duties?
To whom does the clinician owe these duties? If so how best can this dilemma be resolved?
3. Consider the categorical imperatives. Is this a case of respect for autonomy and confidentiality?
If so are there sufficient grounds to ignore her wishes?
4. Application of principles. How might the four key ethical principles of ethical clinical practice
be applied?
What other considerations might apply?
What are your considerations about the best course of action in India? Give your reasons.
27
Public health a consideration of utilitarian ethics
Public health programmes are usually founded on utilitarian grounds of the greatest benefit to the
greatest numbers in terms of 1) combating the spread of disease and 2) cost effectiveness in delivery of
health care. Such programmes are considered justifiable when these benefits greatly outweigh perceived
risks and potential harms. Consider the following current example.
The Human Papilloma Virus is a major cause of cervical cancer. HPV is sexually transmitted with an
estimated 50% of sexually active males and females being infected at some point in their lives. In the
USA, for example, more than 6 million sexually active people are infected with an APV per year. Many
countries are or have introduced a vaccination programme to combat this increasing problem. In the UK
from September 2008 all schoolgirls aged 12-13 will be vaccinated unless their parents specifically
exclude them from the programme (an opt out strategy). Some religious groups have opposed this
because it is seen to be encouraging promiscuity and encouraging unsafe sex.
Consider the utilitarian arguments for and against this programme. In the UK programme parents will be
able to exclude their children from the programme. Others have argued that it should be mandatory for
all children.
In relation to public health, the Utilitarian approach adopts a key principle: when considering one or
more alternative courses of action the right action would be that which produces the greatest benefit to
the greatest number. This formulaic approach is deceptively simple. First identify the benefit and then
measure how many people will benefit from a given action. However, a course of action (A) that
provides benefit to 51% of people but produces significant harm to 20% is not necessarily better than a
course of action (B) which gives benefit to 40% of people but harms only 10%. The extra 11% who may
benefit from action A comes with a heavy price; a significantly greater cost of a further 10% who are
significantly harmed. Nor can we get a simple ethical answer by an arithmetic formula of subtracting
harm from benefit: in A such a calculation produces 31% and in B 30%. The problem is starker if the
people being harmed are not also those receiving any benefit: the benefit to the greater number is here
then at the cost to others. If we are not careful we could justify the enslavement of the few for the benefit
of the many.
Principle of an Equal Consideration of Interests.
One approach to this problem is to hold that for utilitarian principles to apply there must be an equal
consideration of the interests of all in the balance of potential benefit and harm.
Consider again the problem of resuscitating very premature babies presented earlier. In the UK this is
determined on a case by case basis with a clinical assessment of likely outcome. As a consequence
between 20 and 25% of these babies survive with extreme brain damage and profound mental and
physical handicap. In contrast, in Holland the policy is not to resuscitate very premature babies. We
could argue that the cost of the policy in Holland is that 75% of babies who would have survived with
moderate to no handicap but who are by this policy denied a chance of life. We could equally argue that
the cost in the UK for the 75% who survive with little to no handicap is the very profound handicap of
those affected. This demonstrates 1) how difficult it can be to apply the approach of utility to answering
such ethical issues and 2) that there is rarely a clear empirical answer to ethical problems. Also whilst
the actual statistics represent real babies, the extrapolation is that of risk and the potential for harm or
benefit.
28
It is arguable whether it is in the interest of a very sick premature baby who would die naturally and
would not therefore suffer to be resuscitated and kept alive at all costs. But the issue isnt simply
whether it is justified ethically but also who should make the final decision; a question which isnt
readily answered by a utilitarian calculation.
The Utilitarian approach seeks a relatively dispassionate assessment of the consequences of actions or
decisions: that which enhances well-being is good; that which reduces it by producing suffering or pain
is bad. The ethical strives to maximise the good by producing the best balance of benefit and harm. It
forces us to look at all potential consequences of our decisions. A full utilitarian analysis of the
premature baby problem would also consider consequences not only for the babies but also for families,
parents and other siblings, and others in society, although each of these may be given different weights.
The utility analysis of HPV vaccination programme would consider not just the potential advantage to
those vaccinated but also the potential benefits to others in society through reduced demands on scarce
health resources and also the increased productivity resulting from a healthier population; it would also
weigh the potential harm if as critics claim, a vaccination programme encouraged unsafe sex. The
problem as Peter Singer has put it isnt simply whether ends justify means, but which ends sufficiently
justify them
18
.
In practice it is difficult to avoid at least some kind of consequentialist perspective to ethical decisions in
medicine. Even from a deontological view, duty requires a consideration of likely outcome in relation to
fulfilment of that duty. Consider for example the general duty of care, the duty to do that which is in the
best interests of the patient. The major difference in the two approaches in relation to consequence is
that in utilitarian perspectives the ends can be sufficient justification for the means employed. From that
of deontology, the likely ends can only be a measure of how well the duty can be discharged by the
means employed. As we have seen, the categorical imperative of duty sets the ethical threshold that has
to be reached for the imperative to be breeched. There has to be another and significantly conflicting
duty to justify a breech. From a utilitarian perspective confidentiality as a means to an end is
intrinsically neither morally right nor wrong, for the deontologist confidentiality is an end in itself a
duty to be discharged. A strictly utilitarian viewpoint might consider a breech of patient confidentiality
to be justified whenever the benefit to the greater number of others was seen to outweigh the harm to the
patient whose confidentiality is to be broken. From a consideration of duty only exceptional
circumstances would justify such a breech. For example, a general practitioner might consider a breech
of confidentially in relation to a minor where this is in the best interest of the child and there is a
considered duty to protect the child from harm. Equally, in relation to sexual health, a GP might
consider that the minor is competent to give informed consent and to understand the advice being given
and might choose not to inform the parents if this is against the childs wishes. This is clearly a balanced
judgment; a judgment that stems from duties to respect the childs confidence and protecting the child
from harm, or considering the best interests of the child.
Modern medical ethics tends to focus on the individual relationship between physician and patient and
stresses the autonomy and rights of the patient. From a utilitarian perspective any breech of these rights
would be considered harmful but there may be circumstances where an overriding interest for the
welfare of others might be considered to justify compromising autonomy, informed consent or
confidentiality for example, to protect the public from a contagious disease. There may also be a
justification where the overriding consideration is to protect the patient where this cannot be achieved
without a breech of the patients autonomy.
18
Singer, P. Practical Ethics (2
nd
Edition 1993) Cambridge University Press.
29
Clinical Research Ethics
Clinicians may be engaged in research in a variety of ways, both directly and indirectly. Ethical review
and approval should be obtained in all cases of research on human subjects. The primary justification for
research is the expected benefit in improved treatments or prevention of disease. Thus, the justification
is overwhelmingly utilitarian and the ethical judgement involves assessment of likely benefits and
potential harms. All engaged in clinical trials have duties of care and should consider how best these can
be discharged. An ethical approach involves the application of all the tools presented in this course.
Ethical research involving human participants is premised on two fundamental commitments: (1) to
improve human welfare by advancing knowledge and understanding of disease and treatment; but
equally (2) to preserve and protect the dignity and health interests of research participants. Clinical
research aims to benefit individual participants and patient groups through the identification and testing
of improved treatments, and to benefit society by making them widely available. The justification for
human trials of new or potentially improved treatments is usually utilitarian in nature: the potential for a
greater benefit than existing treatments or choices being weighed against the risk of harms.
The potential risk of harm to participants has led to widespread agreement that sound ethical standards
must be observed in clinical research regardless of the perceived benefits
19
. The ends alone, no matter
how good, are insufficient justification for the means employed where they might unduly harm those
involved. This is particularly so when participants are unlikely to be the subsequent beneficiaries, or if
they are likely to carry a substantial burden of risk as participants in such trials. Research involving
human subjects should thus be preceded by careful assessment of predictable risks and burdens in
comparison with foreseeable benefits to the subjects or to others (Helsinki Declaration, article 10.16)
and should only occur if the importance of the objective outweighs the inherent risks and burdens to the
subject (Helsinki Declaration, article 10.18). In this process, informed consent is a fundamental
principle in any research involving human participants; but consent can only be informed if the potential
harms and benefits are clearly understood or, if there is doubt, that the participants understand the nature
of such doubt. It should be clear what the proposed research or intervention might achieve and who will
be the likely beneficiaries.
Consider the following clinical trial:
Epidemiological studies demonstrate a strong correlation between low birth weight and the onset of
cardiovascular disease in later life. Both animal and human studies strongly suggest that maternal
nutrition is an important factor in determining birth weight, in particular a lack of protein in the diet. An
international collaborative team of clinicians and scientists wish to study a cohort of young women in a
rural area of India half of whom will be given a protein supplement to their normal diet, whilst the other
half will receive the same vehicle but without the supplement. The study will be double blinded so that
neither the clinicians nor the women will know which group they belong to. The women will be studied
through to child bearing and the birth weights measured to determine whether the protein enriched diet
increases the birth weights significantly.
Consider the ethical issues that might arise from this proposal.
19
World Medical Association. Declaration of Helisnki: Ethical Principles for Medical Research Involving Human Subjects.
Helsinki, Finland: Adopted by the 18th WMA General Assembly, June 1964.
30
Informed consent from minors - Gillick-competence background to case scenario 2
During the 1980s in England, the Department of Health issued a circular allowing practitioners, under
limited circumstances, to discuss with and apply family planning procedures to minors (<16 years of
age) without the express consent of their parents.
Mrs Gillick, a mother, challenged this in a court of law to get this advice declared illegal. The judgement
in Gillick v West Norfolk and Wisbech Area Health Authority [1984] was in favour of the Health
Authority ruling that a minor was capable of giving consent to contraceptive therapy provided she was
of sufficient mental maturity to understand the implications.
This ruling was overturned by the Court of Appeal on consideration of the duties and rights of parents
and their right to be informed sufficiently to carry out these duties.
The Department of Health with the support of the British Medical Association (representatives of
medical practitioners in the UK) appealed to the House of Lords (The highest appeal court in the UK)
who backed the original judicial decision by a majority of 3:2 allowing practitioners to make a
judgement about the maturity of a minor and to give contraceptive advice and treatment without the
consent of the parents.
The mature minor principle is now commonly referred to as Gillick-competence and is widely
applied in practice, although it is fraught with difficulties.
Essentially a practitioner may be justified in providing advice and treatment without the expressed
consent or knowledge of the parents where:
1) the girl concerned is considered capable of understanding advice
2) she could not be persuaded to inform her parents or to allow the doctor to inform them (implicit
in this is that the practitioner should try to persuade her to inform her parents)
3) she is very likely to have sexual intercourse with or without contraceptive treatment or advice
(withholding such treatment or giving it is unlikely to influence her sexual behaviour)
4) without contraceptive advice or treatment her physical and mental health is likely to suffer (she
is at risk of sexually transmitted disease or may become pregnant)
5) overall it is considered to be in her best interest on the balance of probable benefits and potential
harms.
The obligation is firmly imposed on the doctor to attempt to persuade the girl to inform her parents or to
allow him/her to do so.
This approach is an attempt to act in the best interest of the girl considering that where possible it is
best that parents are involved. It balances this with the right of parents to be informed to carry out the
duty of care to their child. The paramount concern, however, is the best interest and health of the child.
31
Hereditary disease and confidentiality
Consider the case of a young man who has been found to have a hereditary condition but informs his GP
that he does not wish this to be disclosed even to other members of his family who are also patients of
this GP. The practitioner now has information which may be important to these patients. How best can
this situation be resolved?
Confidentiality in relation to genetic information is likely to present a common ethical dilemma as it
becomes possible to screen for gene mutations linked to an increasing number and type of diseases.
Patients may find they have a mutant gene about which they were previously unaware. In many cases
this will be screening for risk of multifactor conditions rather than single-gene-related diseases. Such
risk will not mean that the patient will in due course develop the condition; it simply increases the
possibility of doing so. In other cases, having the mutant gene will mean that the person will certainly
develop the disease.
Genetic information is generally thought to present a particular problem in relation to confidentiality
because if the condition is found in one member of the family it is likely to be found in others and to
affect future offspring in the family. It might therefore be argued that such family members have a right
to be informed so that they are then able to make appropriate informed choices about their health, life-
style and reproduction. Equally, however, they have a right not to be informed.
This presents two major problems for the practitioner: 1) whether to breech the confidentiality of his
patient by informing other members of the family that they may also have the mutant gene; and 2) the
presumption that these patients would wish to be informed. It is not inconceivable that they know
already of the history in the family, but have chosen not to find out whether or not they also carry the
gene. People have different approaches to the Sword of Damocles
20
; some may wish to know for
certain whether they will be affected so that they can come to terms with it in living their lives; others
may wish to live there lives unaffected by such knowledge.
The problem for the doctor if he decides it is in the best interest of other family members that they
should be informed is how this should be done. Simply raising the subject may suggest to the family that
there is a problem and opens Pandoras Box
21
. Following the principle of non-maleficence would
suggest great caution in giving information which may be harmful. Where we saw one dilemma there
are now at least two: whether the confidentiality should be breeched and whether or not more harm than
good is done by informing family members. Arguably, the answer to the latter should at least be certain
before considering whether to breech confidentiality. Another consideration is whether this can be done
without breeching patient confidentiality and anonymity.
One approach to this problem might be for the GP to suggest screening for the gene only where there are
good clinical grounds during a routine consultation. However, this raises the stakes and may create
unnecessary anxiety.
20
Something that threatens to bring imminent disaster: Domocles a figure of ancient Greek legend traded places for a day
with Dionysius, the unpopular ruler of Syracuse, only to find that a sword hovered above his head hanging by a single fine
hair.
21
Pandora, a woman of Greek legend, was sent by the Gods with a jar of evils. She opened the jar, also referred to as a box,
out of curiosity thus releasing the evils into the world. The phrase opening Pandoras box refers to actions taken without
considering the consequences of unforeseen problems over which there will be no control.
32
Several criteria should be fulfilled to justify a breech of confidentiality: 1) there must be a significant
potential harm to the other parties; 2) these parties must be able to act effectively upon such information;
3) it should be clear that the parties would wish to be informed; 4) sufficient counselling should be
available to support the affected parties; and 5) every effort has been made to persuade the patient to
disclose the information or allow it to be disclosed.
33
Conclusion
The aim of this course has been to provide, through a series of workshops, an understanding of medical ethics
and how it is applied in clinical practice.
You should now be able to:
1. describe and discuss the principle strands of ethical thought
2. systematically apply them to ethical dilemmas in clinical practice and how they might best be dealt with
You should also have gained an understanding of and be able to demonstrate in practice
1. Utilitarianism
2. Deontology
3. The Principles approach to medical ethics and how they are applied
4. Autonomy
5. Informed consent
6. Confidentiality
7. Human Rights as applied to medicine
Ethics is not a prescription or set of rules to be followed blindly. There is rarely a single right answer to the
ethical dilemmas in practice, but ethics involves a systematic approach to moral dilemmas. Patients and society
should be confident that difficult choices are not dealt with in an arbitrary fashion, or simply dependent on the
particular moral stand taken by clinicians. Choices should be made or presented fairly and usually in the best
interests of the patient. Ethics is just us much about HOW dilemmas are resolved than with WHAT the right
choices or actions should be. Central to modern clinical ethics is the dignity and respect for the patient as
individuals capable of understanding and where possible taking decisions about their treatment.
The example case scenarios covered in the workshops were designed to give you practice in considering each
case systematically but also considering each case specifically. You will probably not be satisfied that each case
has been resolved ideally. Ethics rarely produces a perfect solution. You will, however, have gained a better
insight into the nature of the dilemmas addressed.
34
Answers to questions:
Which of the following do you consider to be the best description (hint: only one should be picked)?
1. Ethics decides what is right or wrong
2. Ethics decides what is moral
3. Ethics considers the nature of, and how best to deal with conflicts in moral imperatives
The correct answer is 3. Ethics does not decide what is moral. Ethics arises because we have conflicts
between and arising from moral imperatives. Ethics does to an extent decide how best we deal with
these conflicts but it doesnt decide what is right and wrong per se.
Which of the following is true (only one is true)?
1. Deontology is the consideration of duties and obligations
2. Deontology considers the balance of benefits and harms
3. Deontology considers that ends may justify means
The correct answer is 1. Deontology is the consideration or study of duties and obligations. The
discharge of duties may have consequences but the duties exist regardless of these outcomes they are
ends in themselves. A deontology approach considers how best to deal with conflicts of duties, to
whom they are owed and how extensive they are.
Which of the following is true (more than one may be true)?
1. A Utilitarian approach in ethics considers the consequences of actions or choices
2. A Utilitarian approach in ethics considers that ends may justify means
3. A Utilitarian approach in ethics considers whether clinicians have discharged their duties in the best
interests of their patients
Generally both 1 and 2 are the correct. 3 might be considered in utilitarian ethics where best interest is
judged by an assessment of the greatest benefit in relation to harm; although duty in a utilitarian perspective is
usually determined by a consideration of the best outcome i.e. ends justifying means. In contrast deontology
considers duties to exist independently of outcome.
Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Edinburgh Handedness InventoryDocument1 pageEdinburgh Handedness Inventoryandy94264100% (1)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Routine Workplace ProblemsDocument9 pagesRoutine Workplace ProblemsShommer ShotsPas encore d'évaluation
- Wilks Ranch HandbookDocument36 pagesWilks Ranch Handbookapi-316695313Pas encore d'évaluation
- Evidence Before The Southborough Committee PDFDocument31 pagesEvidence Before The Southborough Committee PDFVeeramani ManiPas encore d'évaluation
- ReductionDocument63 pagesReductionwawa3385Pas encore d'évaluation
- Hypertensive RetinopathyDocument5 pagesHypertensive Retinopathywawa3385Pas encore d'évaluation
- NeurovascularDocument10 pagesNeurovascularwawa3385Pas encore d'évaluation
- Start TriageDocument12 pagesStart Triagewawa3385Pas encore d'évaluation
- NeurovascularDocument10 pagesNeurovascularwawa3385Pas encore d'évaluation
- TraksiDocument5 pagesTraksiwawa3385Pas encore d'évaluation
- Pneumothorax SXDocument1 pagePneumothorax SXwawa3385Pas encore d'évaluation
- PnemothoraxDocument1 pagePnemothoraxwawa3385Pas encore d'évaluation
- Anemia SymptomsDocument1 pageAnemia Symptomswawa3385Pas encore d'évaluation
- AnemiaDocument1 pageAnemiawawa3385Pas encore d'évaluation
- PediculosisDocument1 pagePediculosiswawa3385Pas encore d'évaluation
- Causes of AnemiaDocument2 pagesCauses of Anemiawawa3385Pas encore d'évaluation
- EBOLADocument4 pagesEBOLAwawa3385Pas encore d'évaluation
- Anemia: NIH: National Heart, Lung, and Blood InstituteDocument1 pageAnemia: NIH: National Heart, Lung, and Blood Institutewawa3385Pas encore d'évaluation
- Pregnancy - Antenatal Checks of Your Baby: Baby in Vertex - or 'Head' Down PositionDocument4 pagesPregnancy - Antenatal Checks of Your Baby: Baby in Vertex - or 'Head' Down Positionwawa3385Pas encore d'évaluation
- CDC Ebola Fact SheetDocument13 pagesCDC Ebola Fact Sheetيوسف سيمنزPas encore d'évaluation
- Hypertensive RetinopathyDocument5 pagesHypertensive Retinopathywawa3385Pas encore d'évaluation
- Normal Puerperium PDFDocument22 pagesNormal Puerperium PDFwawa3385100% (1)
- Addressing Patients' Emotional and Spiritual Needs: Patient CenterednessDocument12 pagesAddressing Patients' Emotional and Spiritual Needs: Patient Centerednesswawa3385Pas encore d'évaluation
- 1 - NICE Guidelines - FullDocument393 pages1 - NICE Guidelines - FullangiemerazPas encore d'évaluation
- UrethritisDocument2 pagesUrethritiswawa3385Pas encore d'évaluation
- CnoDocument24 pagesCnotherealoneandonlyonePas encore d'évaluation
- CnoDocument24 pagesCnotherealoneandonlyonePas encore d'évaluation
- Yeohee Im Outcome LetterDocument2 pagesYeohee Im Outcome LetterAlanna VagianosPas encore d'évaluation
- Creating Ethical Culture in Six StepsDocument3 pagesCreating Ethical Culture in Six StepsParesh S. SalvePas encore d'évaluation
- The Mathematics of SurvivalDocument48 pagesThe Mathematics of SurvivalEnglish PENPas encore d'évaluation
- For Other Uses, See - Not To Be Confused With .: Merged DiscussDocument19 pagesFor Other Uses, See - Not To Be Confused With .: Merged DiscussMarvin NavaPas encore d'évaluation
- Petitioner Lord Jagannath Memorial State MootDocument11 pagesPetitioner Lord Jagannath Memorial State MootABINASH DASPas encore d'évaluation
- 826 Event Proposal PDFDocument4 pages826 Event Proposal PDFAzaria Naufal TridanadyaksaPas encore d'évaluation
- Hammurabi Laws EssayDocument2 pagesHammurabi Laws EssayRonPas encore d'évaluation
- Kebebasan Memilih Pihak Dalam Kontrak Pada Asas Kebebasan Berkontrak Dalam Sewa Menyewa Kamar TinggalDocument22 pagesKebebasan Memilih Pihak Dalam Kontrak Pada Asas Kebebasan Berkontrak Dalam Sewa Menyewa Kamar Tinggal92 shinerPas encore d'évaluation
- Lecture 2 PragmaticsDocument4 pagesLecture 2 PragmaticsAnonymous QXOdMyslRPas encore d'évaluation
- Cultural Institution PresentationDocument17 pagesCultural Institution PresentationMichael Mao100% (1)
- GAD AnalysisDocument27 pagesGAD AnalysisAnn PulidoPas encore d'évaluation
- Chua-Qua v. Clave (Digest)Document2 pagesChua-Qua v. Clave (Digest)ArahbellsPas encore d'évaluation
- Sociology ProjectDocument17 pagesSociology ProjectSiddarth PrakashPas encore d'évaluation
- LGBTDocument3 pagesLGBTapi-279290977Pas encore d'évaluation
- Prejudice and DiscriminationDocument23 pagesPrejudice and DiscriminationJazyrin M. PullanPas encore d'évaluation
- Department of English ChaitaliDocument5 pagesDepartment of English ChaitaliSaurabh YadavPas encore d'évaluation
- Comparing The Literature of The British IslesDocument2 pagesComparing The Literature of The British IslesArslan Ahmad100% (2)
- Chinua Achebe: by Camille RellosaDocument29 pagesChinua Achebe: by Camille RellosaCamille RellosaPas encore d'évaluation
- GR No 217910 Jesus Nicardo M Falcis III Vs Civil Registrar GeneralDocument31 pagesGR No 217910 Jesus Nicardo M Falcis III Vs Civil Registrar GeneralMikee Angeles67% (3)
- Ethical Issues in Women's EqualityDocument9 pagesEthical Issues in Women's EqualityKomal KapilPas encore d'évaluation
- Social Identity and Intergroup Behaviour-TajfelDocument30 pagesSocial Identity and Intergroup Behaviour-TajfelJuli SerranoPas encore d'évaluation
- UNSCW. United Nations Status On The Commission of WomenDocument19 pagesUNSCW. United Nations Status On The Commission of WomenAbdul RehmanPas encore d'évaluation
- Getting Over Your Fear of Talking About DiversityDocument4 pagesGetting Over Your Fear of Talking About Diversityerumrazvi043Pas encore d'évaluation
- Townsend v. Colorado Department, 10th Cir. (2016)Document3 pagesTownsend v. Colorado Department, 10th Cir. (2016)Scribd Government DocsPas encore d'évaluation
- South African DiscriminationDocument5 pagesSouth African Discriminationmanik birdiPas encore d'évaluation
- The Social Institutions and Gender Index (SIGI) by Keiko NowackaDocument22 pagesThe Social Institutions and Gender Index (SIGI) by Keiko NowackaADBGADPas encore d'évaluation