Vous aimerez peut-être aussi
- Monday, Tuesday, Thursday & Friday: St. Pio of Pietrelcina ChapelDocument2 pagesMonday, Tuesday, Thursday & Friday: St. Pio of Pietrelcina Chapelkristel_nicole18yahoPas encore d'évaluation
- Emergency & DisasterDocument1 pageEmergency & Disasterkristel_nicole18yahoPas encore d'évaluation
- Drug OrderDocument5 pagesDrug Orderkristel_nicole18yahoPas encore d'évaluation
- Diagram I Pathogenesis of Insulin Dependent DM (Type 1) : DiagramsDocument2 pagesDiagram I Pathogenesis of Insulin Dependent DM (Type 1) : Diagramskristel_nicole18yahoPas encore d'évaluation
- Drug StudyDocument8 pagesDrug Studykristel_nicole18yahoPas encore d'évaluation
- Vector Part 2 and 3Document18 pagesVector Part 2 and 3kristel_nicole18yahoPas encore d'évaluation
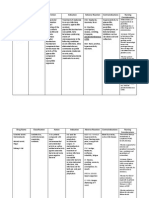
- Drug Name Mechanism of Action Indication Contraindication Side Effects/Adverse Reaction Nursing Responsibility CNS-malaiseDocument3 pagesDrug Name Mechanism of Action Indication Contraindication Side Effects/Adverse Reaction Nursing Responsibility CNS-malaisekristel_nicole18yahoPas encore d'évaluation
- NCPDXDocument3 pagesNCPDXkristel_nicole18yahoPas encore d'évaluation
- Addisons DiseaseDocument1 pageAddisons Diseasekristel_nicole18yahoPas encore d'évaluation
- Drug AnalysisDocument4 pagesDrug Analysiskristel_nicole18yahoPas encore d'évaluation
- 3NCPDocument4 pages3NCPkristel_nicole18yahoPas encore d'évaluation
- Drug AnalysisDocument4 pagesDrug Analysiskristel_nicole18yahoPas encore d'évaluation
- Nursing care plan for post-surgical gastric cancer patientDocument2 pagesNursing care plan for post-surgical gastric cancer patientkristel_nicole18yahoPas encore d'évaluation
- Chemistry Date: 04/29/14: Developed or Changed The Ranges From Her Chemistry LabDocument1 pageChemistry Date: 04/29/14: Developed or Changed The Ranges From Her Chemistry Labkristel_nicole18yahoPas encore d'évaluation
- Social History - Generativity vs StagnationDocument1 pageSocial History - Generativity vs Stagnationkristel_nicole18yahoPas encore d'évaluation
- 3rd NCP Risk For ConstipationDocument2 pages3rd NCP Risk For Constipationkristel_nicole18yaho100% (3)
- Gastric Adenocarcinoma Nursing CareDocument5 pagesGastric Adenocarcinoma Nursing Carekristel_nicole18yahoPas encore d'évaluation
- Addisons DiseaseDocument1 pageAddisons Diseasekristel_nicole18yahoPas encore d'évaluation
- Case Pres NCP HyperthermiaDocument2 pagesCase Pres NCP Hyperthermiakristel_nicole18yahoPas encore d'évaluation
- Drug OrderDocument5 pagesDrug Orderkristel_nicole18yahoPas encore d'évaluation
- Nursing care plan for post-surgical gastric cancer patientDocument2 pagesNursing care plan for post-surgical gastric cancer patientkristel_nicole18yahoPas encore d'évaluation
- Gastric Adenocarcinoma Nursing CareDocument5 pagesGastric Adenocarcinoma Nursing Carekristel_nicole18yahoPas encore d'évaluation
- Clinical Teaching Behavior Student'S Learning Response: Conceptual FrameworkDocument5 pagesClinical Teaching Behavior Student'S Learning Response: Conceptual Frameworkkristel_nicole18yahoPas encore d'évaluation
- DemoDocument6 pagesDemokristel_nicole18yahoPas encore d'évaluation
- Hinds & Gattuso, 1999Document1 pageHinds & Gattuso, 1999kristel_nicole18yahoPas encore d'évaluation
- Case Study PathoDocument4 pagesCase Study Pathokristel_nicole18yahoPas encore d'évaluation
- Hinds & Gattuso, 1999Document1 pageHinds & Gattuso, 1999kristel_nicole18yahoPas encore d'évaluation
- 10 17 1 PB PDFDocument14 pages10 17 1 PB PDFnylorjayPas encore d'évaluation
- Predisposing Factors Precipitating FactorsDocument1 pagePredisposing Factors Precipitating Factorskristel_nicole18yahoPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Gabriel Axel - Master Thesis - Vision The Art of Evolution (2010)Document41 pagesGabriel Axel - Master Thesis - Vision The Art of Evolution (2010)gabrielaxelPas encore d'évaluation
- The List by INDITEX. IV Edition - PDF SetasDocument37 pagesThe List by INDITEX. IV Edition - PDF SetasZOUARIPas encore d'évaluation
- IOL Calculation in Complex Corneal ConditionsDocument8 pagesIOL Calculation in Complex Corneal ConditionsShimaa MersalPas encore d'évaluation
- MANUAL VISIOMETRO VS-V - Universal - Manual - 2015Document23 pagesMANUAL VISIOMETRO VS-V - Universal - Manual - 2015ginalimartinezmuPas encore d'évaluation
- EyetgDocument19 pagesEyetgLissy JyothishPas encore d'évaluation
- Retina: Zarieh Dawn L. Novela Medicine 2Document50 pagesRetina: Zarieh Dawn L. Novela Medicine 2Zari NovelaPas encore d'évaluation
- Glaucoma: Direct Mechanical Theory - Suggests That HighDocument4 pagesGlaucoma: Direct Mechanical Theory - Suggests That HighMarissa AsimPas encore d'évaluation
- Human Eye: General PropertiesDocument10 pagesHuman Eye: General PropertiesVijay RajendiranPas encore d'évaluation
- DFV Diagnostic Product Guide ResourceDocument19 pagesDFV Diagnostic Product Guide ResourceSer NdcPas encore d'évaluation
- Brain Bee 2013 Study Guide FULLDocument12 pagesBrain Bee 2013 Study Guide FULLmsawickaPas encore d'évaluation
- Glaucoma: Pgmi Abadilla Angela MarieDocument29 pagesGlaucoma: Pgmi Abadilla Angela MarieAngel AbadillaPas encore d'évaluation
- Physiology Chapter 1 & 2 ReviewDocument193 pagesPhysiology Chapter 1 & 2 ReviewRichardPas encore d'évaluation
- Human Color Perception: Robert BoyntonDocument2 pagesHuman Color Perception: Robert BoyntonpauloPas encore d'évaluation
- UNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaDocument98 pagesUNIVERSITY OF MEDICAL SCIENCES"REZONANCA"-Halil Ajvazi/Ophthalmology/Prishtina/Republic of KosovaHALIL Z.AJVAZI100% (1)
- Eyestar 900 BrochureDocument16 pagesEyestar 900 BrochureHaag-Streit UK (HS-UK)Pas encore d'évaluation
- 4 Lobes FunctionDocument4 pages4 Lobes FunctionAcharya PradeepPas encore d'évaluation
- Physiology Eye: of TheDocument164 pagesPhysiology Eye: of TheZZ Millania TitahPas encore d'évaluation
- Glaucoma Management and Target IOPDocument24 pagesGlaucoma Management and Target IOPElfi RisalmaPas encore d'évaluation
- Eye diseases: symptoms and conditionsDocument2 pagesEye diseases: symptoms and conditionsRaju ShresthaPas encore d'évaluation
- 13.2 Sense Organ - EyeDocument28 pages13.2 Sense Organ - EyeMuhammad Amin SuhaimiPas encore d'évaluation
- DPL 13 Feb 2023 - All IndiaDocument18 pagesDPL 13 Feb 2023 - All IndiaInfo UcsplPas encore d'évaluation
- Eyes - Ears - Mouth - Nose (Lecture 5)Document50 pagesEyes - Ears - Mouth - Nose (Lecture 5)اسامة محمد السيد رمضانPas encore d'évaluation
- Binocular Vision ScheimanDocument732 pagesBinocular Vision ScheimanOptom Dang100% (1)
- Manual de Técnicas Qx. en Oftalmología 14-10-22Document115 pagesManual de Técnicas Qx. en Oftalmología 14-10-22YAZMIN DEL JESUS LARA HUCHINPas encore d'évaluation
- Color and LightDocument1 pageColor and LightĐức ToànPas encore d'évaluation
- Vocab Quiz-Chap 4-Sens & PercDocument3 pagesVocab Quiz-Chap 4-Sens & PercJanie VandeBergPas encore d'évaluation
- Disturbance in Sensory PerceptionDocument48 pagesDisturbance in Sensory PerceptionKristine Louise JavierPas encore d'évaluation
- Common Retinal Diseases: FloatersDocument7 pagesCommon Retinal Diseases: FloatersDan-Dan Irika CentinoPas encore d'évaluation
- Optic Disc Abnormalities - Cheat SheetDocument6 pagesOptic Disc Abnormalities - Cheat SheetPaula EmyPas encore d'évaluation
- Contact Lenses 1: by Hatem S.H. Barhoom MHSC (Clinical Optometry) UKM - MalaysiaDocument250 pagesContact Lenses 1: by Hatem S.H. Barhoom MHSC (Clinical Optometry) UKM - MalaysiaHasan AnsariPas encore d'évaluation