Vous aimerez peut-être aussi
- Mod Path Ol 2008176 ADocument6 pagesMod Path Ol 2008176 AOkki Masitah Syahfitri NasutionPas encore d'évaluation
- J Path 168001526Document5 pagesJ Path 168001526Surendar KesavanPas encore d'évaluation
- Molecular Analysis To Demonstrate That Odontogenic Keratocysts Are NeoplasticDocument5 pagesMolecular Analysis To Demonstrate That Odontogenic Keratocysts Are NeoplasticSamar KhanPas encore d'évaluation
- CPG Island Hypermethylation-Associated Silencing of Micrornas Promotes Human Endometrial CancerDocument10 pagesCPG Island Hypermethylation-Associated Silencing of Micrornas Promotes Human Endometrial CancerFerdina NidyasariPas encore d'évaluation
- 4442 FullDocument11 pages4442 FullntphquynhPas encore d'évaluation
- 5 Pages Evidence of Fetal Microchimerism in Hashimotos ThyroiditisDocument5 pages5 Pages Evidence of Fetal Microchimerism in Hashimotos ThyroiditisKristinDaiglePas encore d'évaluation
- Supplemental DataRevisedDocument12 pagesSupplemental DataRevisedCezary TomczykPas encore d'évaluation
- Jcinvest00043 0362Document8 pagesJcinvest00043 0362api-26848049Pas encore d'évaluation
- 236 - Spectral Karyotyping of The Human Colon Cancer Cell Lines SW480 and SW620Document8 pages236 - Spectral Karyotyping of The Human Colon Cancer Cell Lines SW480 and SW620Fran MoyaPas encore d'évaluation
- MMP10 NSCLCDocument9 pagesMMP10 NSCLCbhaskarPas encore d'évaluation
- International Journal of Cancer Volume 85 Issue 3 2000Document8 pagesInternational Journal of Cancer Volume 85 Issue 3 2000BenePicarPas encore d'évaluation
- Prognostic Significance of Er, PR, Ki67, C-Erbb-2, and P53 in Endometrial CarcinomaDocument7 pagesPrognostic Significance of Er, PR, Ki67, C-Erbb-2, and P53 in Endometrial CarcinomabertinelwanPas encore d'évaluation
- Equine Yolk Sac: A Stem Cells Source: Saco Vitelino Equino: Una Fuente de Células MadreDocument9 pagesEquine Yolk Sac: A Stem Cells Source: Saco Vitelino Equino: Una Fuente de Células MadreisabelPas encore d'évaluation
- PC3 ClineDocument6 pagesPC3 ClineANGEL SAUL SERRANO ANGULOPas encore d'évaluation
- Ijcep0007 0602Document9 pagesIjcep0007 0602Deedee RenovaldiPas encore d'évaluation
- Doença de Batten 2004Document9 pagesDoença de Batten 2004Ana Paula BoscatoPas encore d'évaluation
- Introduction Cancer Is Abnormal Cell Growth That Proliferates in An Uncontrolled Pattern That Allows It To Continue and SpreadDocument10 pagesIntroduction Cancer Is Abnormal Cell Growth That Proliferates in An Uncontrolled Pattern That Allows It To Continue and SpreadmrlakshyaranaPas encore d'évaluation
- Citosol (Thiamylal Sodium) Triggers Apoptosis and Affects Gene Expressions of Murine Leukemia RAW 264.7 Cells - RS-C Wu, C-S Yu, 2Document1 pageCitosol (Thiamylal Sodium) Triggers Apoptosis and Affects Gene Expressions of Murine Leukemia RAW 264.7 Cells - RS-C Wu, C-S Yu, 2Alondra MaldonadoPas encore d'évaluation
- Effects of Cordyceps Militaris Extract On Tumor ImmunitDocument18 pagesEffects of Cordyceps Militaris Extract On Tumor Immunitqueenienguyen2609Pas encore d'évaluation
- Citosol (Thiamylal Sodium) Triggers Apoptosis and Affects Gene Expressions of Murine Leukemia RAW 264.7 Cells - RS-C Wu, C-S YuDocument1 pageCitosol (Thiamylal Sodium) Triggers Apoptosis and Affects Gene Expressions of Murine Leukemia RAW 264.7 Cells - RS-C Wu, C-S YuAlondra MaldonadoPas encore d'évaluation
- 2012 MC Proteomics - Proteomics and Transcriptomics Approach To Identify Leukemic Stem Cell MarkersDocument34 pages2012 MC Proteomics - Proteomics and Transcriptomics Approach To Identify Leukemic Stem Cell MarkersJosé Nivaldo Ifatunmibi Aworeni OdusolaPas encore d'évaluation
- Citotoxic CAPEDocument8 pagesCitotoxic CAPEannisa_yuniartiPas encore d'évaluation
- CMJ 55 3 Kit 24891284Document6 pagesCMJ 55 3 Kit 24891284Mihaela-Alexandra PopPas encore d'évaluation
- 15-Li Chen (531-538)Document8 pages15-Li Chen (531-538)Nguyễn Thanh TùngPas encore d'évaluation
- Analysis of Gene Expression in Cancer Cell Lines Identifies Candidate Markers For Pancreatic Tumorigenesis and MetastasisDocument13 pagesAnalysis of Gene Expression in Cancer Cell Lines Identifies Candidate Markers For Pancreatic Tumorigenesis and MetastasisAbhishek BardhanPas encore d'évaluation
- Ramalingam - ArticleDocument9 pagesRamalingam - ArticleCaro FrairePas encore d'évaluation
- Cyclooxygenase-2 OverexpressionDocument7 pagesCyclooxygenase-2 OverexpressionGessyca JeyPas encore d'évaluation
- A Combined Artificial Chromosome Stem Cell Therapy Method in A Model Experiment Aimed at The Treatment of Krabbes Disease in The Twitcher Mouse CMLS 2008Document9 pagesA Combined Artificial Chromosome Stem Cell Therapy Method in A Model Experiment Aimed at The Treatment of Krabbes Disease in The Twitcher Mouse CMLS 2008Robert KatonaPas encore d'évaluation
- Food and Chemical Toxicology: Kyoung Jin Nho, Jin Mi Chun, Ho Kyoung KimDocument10 pagesFood and Chemical Toxicology: Kyoung Jin Nho, Jin Mi Chun, Ho Kyoung KimMd Jahidul IslamPas encore d'évaluation
- MUC1 Expression in Human Prostate Cancer Cell Lines and Primary TumorsDocument9 pagesMUC1 Expression in Human Prostate Cancer Cell Lines and Primary TumorsInesaPas encore d'évaluation
- A New Approach To Immunological Sexing of Sperm Blecher 1999Document13 pagesA New Approach To Immunological Sexing of Sperm Blecher 1999Sergio L.Pas encore d'évaluation
- Head NeckDocument9 pagesHead NeckAjeet AmbujPas encore d'évaluation
- VeselyDocument7 pagesVeselyhitherehiPas encore d'évaluation
- Integrative CUT&Tag-RNA-Seq Analysis of Histone Variant macroH2A1-dependent Orchestration of Human Induced Pluripotent Stem Cell ReprogrammingDocument16 pagesIntegrative CUT&Tag-RNA-Seq Analysis of Histone Variant macroH2A1-dependent Orchestration of Human Induced Pluripotent Stem Cell Reprogrammingniccolo.liorni1Pas encore d'évaluation
- The Multistage Process of Carcinogenesis in Human Esophageal Epithelial Cells Induced by Human PapillomavirusDocument8 pagesThe Multistage Process of Carcinogenesis in Human Esophageal Epithelial Cells Induced by Human PapillomavirusIlma Kurnia SariPas encore d'évaluation
- 10.33073 - PJM 2022 023Document6 pages10.33073 - PJM 2022 023Andy SetiawanPas encore d'évaluation
- Gene Expression Profiling of Human Decidual Macrophages Evidence For Immunosuppressive PhenotypeDocument9 pagesGene Expression Profiling of Human Decidual Macrophages Evidence For Immunosuppressive PhenotypeCristian Gutiérrez VeraPas encore d'évaluation
- Cancer-Associated Adipocytes Promote The Invasion and Metastasis in Breast Cancer Through LIFCXCLs Positive Feedback Loop Ayesha MudassarDocument35 pagesCancer-Associated Adipocytes Promote The Invasion and Metastasis in Breast Cancer Through LIFCXCLs Positive Feedback Loop Ayesha MudassarAyesha MudassarPas encore d'évaluation
- Polymorphisms in The Promoter Regions of The Matrix Metalloproteinases-7, - 9 and The Risk of Endometriosis and AdenomyosisDocument5 pagesPolymorphisms in The Promoter Regions of The Matrix Metalloproteinases-7, - 9 and The Risk of Endometriosis and AdenomyosisAndy WijayaPas encore d'évaluation
- Piriformis SyndromeDocument6 pagesPiriformis SyndromeDyan Riza Indah TamiPas encore d'évaluation
- Epidermidis Carrying Biofilm Formation GenesDocument5 pagesEpidermidis Carrying Biofilm Formation GenesLini MaliqisnayantiPas encore d'évaluation
- Cisplatin Cell Cicle ArrestDocument7 pagesCisplatin Cell Cicle ArrestGabriele KrausePas encore d'évaluation
- X - Evaluation - of - Distinct - Freezing - MethodsDocument10 pagesX - Evaluation - of - Distinct - Freezing - Methodsayisha.maharramovaPas encore d'évaluation
- Amer. J. Pathol.-2002-Urist-1199-1206Document8 pagesAmer. J. Pathol.-2002-Urist-1199-1206Charles J. DiComo, PhDPas encore d'évaluation
- Ertao 2016Document7 pagesErtao 2016chemistpl420Pas encore d'évaluation
- 2538 FullDocument6 pages2538 FullAdelyna AndreiPas encore d'évaluation
- Expression of Sox2 in Human Cervical Carcinogenesis: Jing Ji PHD, Peng-Sheng Zheng MD, PHDDocument10 pagesExpression of Sox2 in Human Cervical Carcinogenesis: Jing Ji PHD, Peng-Sheng Zheng MD, PHDAini SavinaPas encore d'évaluation
- Research Article: The c-MYC Protooncogene Expression in CholesteatomaDocument7 pagesResearch Article: The c-MYC Protooncogene Expression in CholesteatomaVicky G OeiPas encore d'évaluation
- Antikanker 3Document5 pagesAntikanker 3Namira NaaziahPas encore d'évaluation
- Resistance in Human Cervical Tumor Cells: Ercc1 Expression As A Molecular Marker of CisplatinDocument5 pagesResistance in Human Cervical Tumor Cells: Ercc1 Expression As A Molecular Marker of CisplatinAmanda Kelly N. MendonçaPas encore d'évaluation
- Supplemetary MaterialDocument5 pagesSupplemetary MaterialAnaPas encore d'évaluation
- Or 26 1 185 PDFDocument7 pagesOr 26 1 185 PDFRoland_IIPas encore d'évaluation
- Hongzhuan Xuan, Zhen Li, Haiyue Yan, Qing Sang, Kai Wang, Qingtao He, Yuanjun WangDocument29 pagesHongzhuan Xuan, Zhen Li, Haiyue Yan, Qing Sang, Kai Wang, Qingtao He, Yuanjun WangTim WongPas encore d'évaluation
- In Vitro Post-Meiotic Germ Cell Development From Human Embryonic Stem CellsDocument10 pagesIn Vitro Post-Meiotic Germ Cell Development From Human Embryonic Stem Cellsucich23Pas encore d'évaluation
- Surgical Endoscopy Sept.1997Document91 pagesSurgical Endoscopy Sept.1997Saibo BoldsaikhanPas encore d'évaluation
- Blood Imp 5Document10 pagesBlood Imp 5ashokPas encore d'évaluation
- 2015 Molecular KlimstraDocument7 pages2015 Molecular KlimstramaomaochongPas encore d'évaluation
- Dna LoadingDocument6 pagesDna LoadingSameer SachdevaPas encore d'évaluation
- 2010 BaxterDocument7 pages2010 BaxtercandiddreamsPas encore d'évaluation
- Best Television SeriesDocument37 pagesBest Television SeriescandiddreamsPas encore d'évaluation
- MesotheliomaDocument7 pagesMesotheliomacandiddreamsPas encore d'évaluation
- Polymorphous Breast CA.Document6 pagesPolymorphous Breast CA.candiddreamsPas encore d'évaluation
- Combined Set of Kaplan 900 and High Frequency Words PDFDocument17 pagesCombined Set of Kaplan 900 and High Frequency Words PDFcandiddreams100% (2)
- 7 Restaurants Worth Visiting in KolkataDocument5 pages7 Restaurants Worth Visiting in KolkatacandiddreamsPas encore d'évaluation
- NeuroendoDocument8 pagesNeuroendocandiddreamsPas encore d'évaluation
- Meningioma SDocument10 pagesMeningioma ScandiddreamsPas encore d'évaluation
- LeiomyomaDocument3 pagesLeiomyomacandiddreamsPas encore d'évaluation
- Hyperplastic Gastric PolypDocument5 pagesHyperplastic Gastric PolypcandiddreamsPas encore d'évaluation
- Male Breast CA.Document6 pagesMale Breast CA.candiddreamsPas encore d'évaluation
- Primary Intracranial Leiomyoma: A Case Report and Literature ReviewDocument3 pagesPrimary Intracranial Leiomyoma: A Case Report and Literature ReviewcandiddreamsPas encore d'évaluation
- Lung OsteomaDocument4 pagesLung OsteomacandiddreamsPas encore d'évaluation
- Current Practice of Gleason Grading of Prostate Carcinoma: ReviewarticleDocument8 pagesCurrent Practice of Gleason Grading of Prostate Carcinoma: ReviewarticlecandiddreamsPas encore d'évaluation
- Validation Cell AnalyzersDocument45 pagesValidation Cell AnalyzerscandiddreamsPas encore d'évaluation
- Hepatic Collision TumourDocument6 pagesHepatic Collision TumourcandiddreamsPas encore d'évaluation
- Eye AstrocytomaDocument5 pagesEye AstrocytomacandiddreamsPas encore d'évaluation
- BreastDocument3 pagesBreastcandiddreamsPas encore d'évaluation
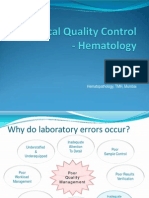
- Statistical Approach in HematologyDocument33 pagesStatistical Approach in HematologycandiddreamsPas encore d'évaluation
- Gastric CancerDocument8 pagesGastric CancercandiddreamsPas encore d'évaluation
- AtherosclerosisDocument8 pagesAtherosclerosiscandiddreamsPas encore d'évaluation
- TMH PBS PresentationDocument61 pagesTMH PBS PresentationcandiddreamsPas encore d'évaluation
- Apocrine Breast LesionsDocument7 pagesApocrine Breast LesionscandiddreamsPas encore d'évaluation
- Clonality Analysis in Hematolymphoid Malignancies: DR Jay MehtaDocument65 pagesClonality Analysis in Hematolymphoid Malignancies: DR Jay MehtacandiddreamsPas encore d'évaluation
- Mean Normal Prothombin Time (MNPT)Document10 pagesMean Normal Prothombin Time (MNPT)candiddreamsPas encore d'évaluation
- MANI Quality Control in Hematology AnalysersDocument65 pagesMANI Quality Control in Hematology Analyserscandiddreams100% (1)
- Normal Hematolymphoid TissuesDocument182 pagesNormal Hematolymphoid TissuescandiddreamsPas encore d'évaluation
- Statistical Approach in HematologyDocument33 pagesStatistical Approach in HematologycandiddreamsPas encore d'évaluation
- Gujral FCMDocument102 pagesGujral FCMcandiddreamsPas encore d'évaluation
- IGCSE Bio Lesson Plan 7 Chemical CoordinationDocument2 pagesIGCSE Bio Lesson Plan 7 Chemical CoordinationHisokagenPas encore d'évaluation
- Linkage Practial ExerciseDocument7 pagesLinkage Practial ExerciseSabesan TPas encore d'évaluation
- College of Nursing All India Instutite of Medical Sciences, Rishikesh (Uttarakhand) B.Sc. (Hons) Nursing 3 Year Batch - 2016 End Term Examination - 2019 Subject - Maternal Health NursingDocument24 pagesCollege of Nursing All India Instutite of Medical Sciences, Rishikesh (Uttarakhand) B.Sc. (Hons) Nursing 3 Year Batch - 2016 End Term Examination - 2019 Subject - Maternal Health NursingRajaPas encore d'évaluation
- MTP Act 1971Document10 pagesMTP Act 1971Dr. Rakshit SolankiPas encore d'évaluation
- National Population PolicyDocument44 pagesNational Population PolicyKrishnaveni MurugeshPas encore d'évaluation
- The Ultra So No Graphic Diagnosis of Pregnancy in The Dog and Cat NotesDocument8 pagesThe Ultra So No Graphic Diagnosis of Pregnancy in The Dog and Cat NotesAnur SinglaPas encore d'évaluation
- Detailed Study On Infertility Its Causes and TreatmentDocument2 pagesDetailed Study On Infertility Its Causes and TreatmentBibhuti bhusan MondalPas encore d'évaluation
- Multiple Pregnancy PDFDocument12 pagesMultiple Pregnancy PDFHaidar AmrPas encore d'évaluation
- Examination and Processing of Human Semen OMSDocument287 pagesExamination and Processing of Human Semen OMSGerman CabezasPas encore d'évaluation
- Management of Placenta Previa - UpToDateDocument15 pagesManagement of Placenta Previa - UpToDateJuanPulgarínPas encore d'évaluation
- Case Study - OTITIS MEDIADocument9 pagesCase Study - OTITIS MEDIAHasing Amado100% (1)
- Kebo 104Document23 pagesKebo 104ABDUL HADIPas encore d'évaluation
- TheHeidornReport MerchResearch Vol078 ChristianHeidornDocument69 pagesTheHeidornReport MerchResearch Vol078 ChristianHeidornostojicvPas encore d'évaluation
- Premature Rupture of MembranesDocument5 pagesPremature Rupture of MembranesJoselyn San MiguelPas encore d'évaluation
- Acute Scrotal Swelling & Pain in ChildrenDocument58 pagesAcute Scrotal Swelling & Pain in ChildrenalaaPas encore d'évaluation
- Male Hypogonadism - Jarunee - ppt2085280427Document27 pagesMale Hypogonadism - Jarunee - ppt2085280427Melissa Aina Mohd YusofPas encore d'évaluation
- Nkosazane Yomzulu My JourneyDocument324 pagesNkosazane Yomzulu My JourneymbaliPas encore d'évaluation
- Sex EduDocument3 pagesSex EduVarEedt Kodox'sPas encore d'évaluation
- Growing Plants / GerminationDocument62 pagesGrowing Plants / GerminationJulia Katrina RoxasPas encore d'évaluation
- History and Contemporary Perspective of ObstetricDocument5 pagesHistory and Contemporary Perspective of ObstetricRicha KohliPas encore d'évaluation
- January 2011 QP - Unit 2 Edexcel Biology A-LevelDocument20 pagesJanuary 2011 QP - Unit 2 Edexcel Biology A-LevelNiranjan BhuvanaratnamPas encore d'évaluation
- Pregnant Abdomen ExamDocument4 pagesPregnant Abdomen ExamAmiel Francisco ReyesPas encore d'évaluation
- Handout+Step+2+OB+Sakala+Jan+2014.ppt4+ (1) - Part 1 PDFDocument11 pagesHandout+Step+2+OB+Sakala+Jan+2014.ppt4+ (1) - Part 1 PDFMohammad AlHamdany100% (2)
- EpididymitisDocument8 pagesEpididymitisShafira WidiaPas encore d'évaluation
- MCN MidtermDocument3 pagesMCN MidtermPaul Jhon Vergara67% (3)
- The Management of Asherman Syndrome: A Review of LiteratureDocument11 pagesThe Management of Asherman Syndrome: A Review of LiteratureEuphra Adellheid100% (1)
- Slide PUADocument55 pagesSlide PUAWinda LiraPas encore d'évaluation
- Between The Backbone and The Ribs AL QURAN PHENOMENON PDFDocument3 pagesBetween The Backbone and The Ribs AL QURAN PHENOMENON PDFAnonymous SQNcItqXQnPas encore d'évaluation
- Marc Forchetti - Frog Dissection Virtual LabDocument7 pagesMarc Forchetti - Frog Dissection Virtual LabMARCTHEWIZARD08Pas encore d'évaluation
- Health Talk On Antenatl ExerciseDocument12 pagesHealth Talk On Antenatl ExerciseRavina Patel75% (12)