Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Hawke, Morgan - Queen of Dragons Sorceress SeductionDocument29 pagesHawke, Morgan - Queen of Dragons Sorceress SeductionPaula Schneider100% (2)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- HawkDocument5 pagesHawkhemanta saikia100% (2)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Ferlinghetti Lawrence A Coney Island of The MindDocument48 pagesFerlinghetti Lawrence A Coney Island of The MindDengel dabbebi100% (4)
- Savage Worlds - Hellfrost - HeraldryDocument1 pageSavage Worlds - Hellfrost - HeraldryJRSPas encore d'évaluation
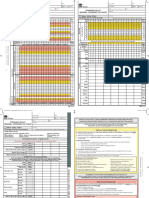
- SAGO AdultObsDocument2 pagesSAGO AdultObsTim BrownPas encore d'évaluation
- Science3 - q2 - m4 Edited KoDocument12 pagesScience3 - q2 - m4 Edited KoZosima Abalos100% (1)
- Excretory Products and Their EliminationDocument9 pagesExcretory Products and Their EliminationBiju MylachalPas encore d'évaluation
- Worm Farming With MealwormsDocument1 pageWorm Farming With MealwormsVenketeshwar SwamiPas encore d'évaluation
- LPTDocument15 pagesLPTShikha SharmaPas encore d'évaluation
- Excretory System of ChickenDocument3 pagesExcretory System of ChickenAjikPas encore d'évaluation
- U.S. Seafood Exports Top MarketsDocument8 pagesU.S. Seafood Exports Top Marketssachin_microPas encore d'évaluation
- An Incident by Anton Pavlovich ChekhovDocument5 pagesAn Incident by Anton Pavlovich Chekhovapi-19787590Pas encore d'évaluation
- Toxicological Effects of Extracts of The Leaves of Scoparia Dulcis On The Brain ofDocument5 pagesToxicological Effects of Extracts of The Leaves of Scoparia Dulcis On The Brain ofFrancis AbuludePas encore d'évaluation
- Dukan Diet Food ListDocument2 pagesDukan Diet Food ListprogramgrabberPas encore d'évaluation
- Science Grade 3 Life Unit 3L1Document22 pagesScience Grade 3 Life Unit 3L1Cristina Isabel Saavedra CuellesPas encore d'évaluation
- Androgenic Effect On Secondary Male CharacteristicsDocument7 pagesAndrogenic Effect On Secondary Male CharacteristicsSolaire SunbroPas encore d'évaluation
- Behavioral and Motivational Mechanisms of The BrainDocument58 pagesBehavioral and Motivational Mechanisms of The BrainLarry TongPas encore d'évaluation
- DystociaDocument6 pagesDystociasarguss14100% (2)
- Pakistan Customs Tariff 2014-15Document348 pagesPakistan Customs Tariff 2014-15Kashar KhanPas encore d'évaluation
- 150+ Art Careers - The Ultimate ListDocument28 pages150+ Art Careers - The Ultimate ListJanePas encore d'évaluation
- Curriculum Guide: Magdev Major in Animal Production: Title and Description of Courses UnitsDocument2 pagesCurriculum Guide: Magdev Major in Animal Production: Title and Description of Courses UnitsRomel gonzagaPas encore d'évaluation
- Parts of Speech AssignmentDocument2 pagesParts of Speech Assignmentroyce542Pas encore d'évaluation
- VMR & IbsDocument7 pagesVMR & Ibsnovianti alfinaPas encore d'évaluation
- Dog GoldendoodleDocument8 pagesDog GoldendoodlejustasPas encore d'évaluation
- Report Text TurtleDocument6 pagesReport Text TurtleNadia Aisy-yaya100% (1)
- Grammar ExercisesDocument16 pagesGrammar Exercisesrahimi67100% (2)
- Spellcaster #7Document70 pagesSpellcaster #7nispotulmiPas encore d'évaluation
- Optimal Sizing of Counterflow Cooler For PelletsDocument72 pagesOptimal Sizing of Counterflow Cooler For PelletsChristian MavarezPas encore d'évaluation
- Jesse Bernstein - Selected WorksDocument54 pagesJesse Bernstein - Selected WorksThamyris JonesPas encore d'évaluation
- Lesson 4 Nervous SystemDocument2 pagesLesson 4 Nervous SystemMohammad FalkayPas encore d'évaluation