Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Screener Saham 2 AgustusDocument4 pagesScreener Saham 2 AgustusMuhammad Ikhlas YasinPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- MCOR Bank Windu Kentjana International Tbk Company ReportDocument3 pagesMCOR Bank Windu Kentjana International Tbk Company ReportMuhammad Ikhlas YasinPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Case Report of Hernia Inguinalis Lateralis ReponibleDocument23 pagesCase Report of Hernia Inguinalis Lateralis ReponibleMuhammad Ikhlas YasinPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Physiology CVS ReviewDocument24 pagesPhysiology CVS ReviewkakuPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- 06 Epidemiology of Hypertension PDFDocument2 pages06 Epidemiology of Hypertension PDFHolly JonesPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Physiology GI ReviewDocument13 pagesPhysiology GI ReviewkakuPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Treatment of Hypertension: JNC 8 and More: Pharmacist'S Letter / Prescriber'S LetterDocument6 pagesTreatment of Hypertension: JNC 8 and More: Pharmacist'S Letter / Prescriber'S LetterJen CanlasPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- 925 FullDocument13 pages925 FullMuhammad Ikhlas YasinPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- US Hypertension Management Guidelines: A Review of The Recent Past and Recommendations For The FutureDocument12 pagesUS Hypertension Management Guidelines: A Review of The Recent Past and Recommendations For The Futureirvan121Pas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- Hiv/Aids: Dr. M. Ikhlas YakinDocument9 pagesHiv/Aids: Dr. M. Ikhlas YakinMuhammad Ikhlas YasinPas encore d'évaluation
- Tech AnalDocument64 pagesTech Analjvinod2025Pas encore d'évaluation
- Case Report of Gout ArthritisDocument27 pagesCase Report of Gout ArthritisMuhammad Ikhlas YasinPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Adolescent Medicine IDocument45 pagesAdolescent Medicine Iapi-3712326100% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Physiology GI ReviewDocument13 pagesPhysiology GI ReviewkakuPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Clinical Use of BloodDocument221 pagesClinical Use of BloodRizma Adlia100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Infectious DiseasesDocument30 pagesInfectious DiseasesMuhammad Ikhlas YasinPas encore d'évaluation
- Blood and Blood Transfusion - 0727916572Document96 pagesBlood and Blood Transfusion - 0727916572128551986Pas encore d'évaluation
- Current Clinical Strategies, Handbook of Psychiatric Drugs (2005) - BM OCR 7.0-2.5Document68 pagesCurrent Clinical Strategies, Handbook of Psychiatric Drugs (2005) - BM OCR 7.0-2.5Adina VarzaruPas encore d'évaluation
- To Prevent and Decrease Overweight and Obesity, 2001Document39 pagesTo Prevent and Decrease Overweight and Obesity, 2001Muhammad Ikhlas YasinPas encore d'évaluation
- Assesment of Nutritional Status in Emergency-Affected PopulationsDocument28 pagesAssesment of Nutritional Status in Emergency-Affected PopulationsIrma ArmiyahPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Neuroblastoma PDocument14 pagesNeuroblastoma PMuhammad Ikhlas YasinPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
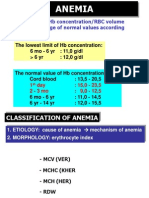
- Reduction of HB concentration/RBC Volume Below The Range of Normal Values According To Age & SexDocument7 pagesReduction of HB concentration/RBC Volume Below The Range of Normal Values According To Age & SexMuhammad Ikhlas YasinPas encore d'évaluation
- Hirschsprung's DiseaseDocument4 pagesHirschsprung's DiseaseNikolaus TalloPas encore d'évaluation
- Weight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Document1 pageWeight-For-Length GIRLS: Birth To 2 Years (Z-Scores)Malisa LukmanPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Childhood CancerDocument12 pagesChildhood CancerMuhammad Ikhlas YasinPas encore d'évaluation
- Leonardo Da VincidsagaDocument39 pagesLeonardo Da VincidsagaMuhammad Ikhlas YasinPas encore d'évaluation
- ATLSDocument5 pagesATLSAnonymous QguKQDpNPas encore d'évaluation
- Acute Nephritic Syndrome (Ans) : Clinical FeaturesDocument8 pagesAcute Nephritic Syndrome (Ans) : Clinical FeaturesMuhammad Ikhlas YasinPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Schonlein Henoch SyndromeDocument12 pagesSchonlein Henoch SyndromeMuhammad Ikhlas YasinPas encore d'évaluation
- ERS M22 PC4 FerryDocument2 pagesERS M22 PC4 FerryouakgoodPas encore d'évaluation
- AAR Maintenance 001Document3 pagesAAR Maintenance 001prakash reddyPas encore d'évaluation
- Cfm56-3 Engine Regulation by CFMDocument43 pagesCfm56-3 Engine Regulation by CFMnono92100% (5)
- Bs8161 - Chemistry Laboratory Syllabus: Course ObjectivesDocument47 pagesBs8161 - Chemistry Laboratory Syllabus: Course ObjectiveslevisPas encore d'évaluation
- Growth Developt Pearl MilletDocument17 pagesGrowth Developt Pearl MilletdarmaPas encore d'évaluation
- Tugas B InggrisDocument9 pagesTugas B InggrisDellyna AlmaPas encore d'évaluation
- Wastewater Treatment Plant Design PDFDocument68 pagesWastewater Treatment Plant Design PDFmostafa1alaahobaPas encore d'évaluation
- FB77 Fish HatcheriesDocument6 pagesFB77 Fish HatcheriesFlorida Fish and Wildlife Conservation CommissionPas encore d'évaluation
- WSO 2022 IB Working Conditions SurveyDocument42 pagesWSO 2022 IB Working Conditions SurveyPhạm Hồng HuếPas encore d'évaluation
- Female Reproductive System Histology IDocument5 pagesFemale Reproductive System Histology ISolomon Seth SallforsPas encore d'évaluation
- TS4-F - Fire SafetyDocument2 pagesTS4-F - Fire SafetyDominic SantiagoPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- ME JBP 70A Pen Dissolved Oxygen Meter PDFDocument1 pageME JBP 70A Pen Dissolved Oxygen Meter PDFpiknikmonsterPas encore d'évaluation
- LH 11 180 190 220 230 270 280 390 400 Breaker Safety & Operating InstructionsDocument304 pagesLH 11 180 190 220 230 270 280 390 400 Breaker Safety & Operating InstructionshadensandorPas encore d'évaluation
- Copia de Tissue Response To Dental CariesDocument7 pagesCopia de Tissue Response To Dental Cariesjorefe12Pas encore d'évaluation
- Lesson 1 CA 3Document13 pagesLesson 1 CA 3myndlePas encore d'évaluation
- Đề Thi Thử THPT 2021 - Tiếng Anh - GV Vũ Thị Mai Phương - Đề 13 - Có Lời GiảiDocument17 pagesĐề Thi Thử THPT 2021 - Tiếng Anh - GV Vũ Thị Mai Phương - Đề 13 - Có Lời GiảiHanh YenPas encore d'évaluation
- How To Practice Self Care - WikiHowDocument7 pagesHow To Practice Self Care - WikiHowВасе АнѓелескиPas encore d'évaluation
- Rreinforcement Pad Leak Test ProcedureDocument5 pagesRreinforcement Pad Leak Test ProcedureAmin Thabet100% (2)
- Investigating Population Growth SimulationDocument11 pagesInvestigating Population Growth Simulationapi-3823725640% (3)
- SCE Research Paper PDFDocument12 pagesSCE Research Paper PDFmuoi2002Pas encore d'évaluation
- Auditor General Insurance Regulation Dec 2011Document23 pagesAuditor General Insurance Regulation Dec 2011Omar Ha-RedeyePas encore d'évaluation
- Comm Part For A320Document1 pageComm Part For A320ODOSPas encore d'évaluation
- Lease Practice QuestionsDocument4 pagesLease Practice QuestionsAbdul SamiPas encore d'évaluation
- Abstract - Tropen Tag 2011 PDFDocument634 pagesAbstract - Tropen Tag 2011 PDFzmoghesPas encore d'évaluation
- Nitric OxideDocument20 pagesNitric OxideGanesh V GaonkarPas encore d'évaluation
- Reading and Listening 2Document4 pagesReading and Listening 2Hải Anh TạPas encore d'évaluation
- Roadblocks Overcome Cruise PurchaseTITLE Top 15 Cruise Hesitations Answered TITLE How to Convince People Cruises Worth CostDocument4 pagesRoadblocks Overcome Cruise PurchaseTITLE Top 15 Cruise Hesitations Answered TITLE How to Convince People Cruises Worth CostJanel Castillo Balbiran33% (3)
- Sigma monitor relayDocument32 pagesSigma monitor relayEdwin Oria EspinozaPas encore d'évaluation
- InjectorDocument23 pagesInjectorBac Nguyen100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisD'EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (13)