Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- GlobalTennis Groundstroke Tennis Drills EbookDocument64 pagesGlobalTennis Groundstroke Tennis Drills EbookErick Varela100% (1)
- Tab B Sportsfestguidelines & MechanicsDocument5 pagesTab B Sportsfestguidelines & Mechanicsmaribel de lunaPas encore d'évaluation
- Sports Lesson PlanDocument9 pagesSports Lesson PlanUrška KlasincPas encore d'évaluation
- BWF Coach Manual Level 2 EnglishDocument247 pagesBWF Coach Manual Level 2 Englishafifatul jannahPas encore d'évaluation
- Badminton Umpire Training ManualDocument122 pagesBadminton Umpire Training Manualsweetfever75% (4)
- Sorsogon National Highschool Intramurals 2019Document5 pagesSorsogon National Highschool Intramurals 2019Sylvia-Chan SylveonPas encore d'évaluation
- Sports, Entertainment and Media Marketing A: Individual Assignment - 1 Abhinav Yadav 0385/55Document20 pagesSports, Entertainment and Media Marketing A: Individual Assignment - 1 Abhinav Yadav 0385/55Abhinav YadavPas encore d'évaluation
- SPORTSDocument6 pagesSPORTSRebeca S.OrcalesPas encore d'évaluation
- Sports: Sports Is Classified IntoDocument2 pagesSports: Sports Is Classified IntoTrisha GarciaPas encore d'évaluation
- Sepak TakrawDocument3 pagesSepak TakrawHazim Calixto LimmayogPas encore d'évaluation
- Running Secondary School Sport Participation TrendsDocument20 pagesRunning Secondary School Sport Participation TrendsHanna Relator DolorPas encore d'évaluation
- A Project Report On Badminton History And ChampionshipsDocument20 pagesA Project Report On Badminton History And ChampionshipsManish Vyas38% (13)
- Speakout DVD Extra Intermediate Unit 07 PDFDocument1 pageSpeakout DVD Extra Intermediate Unit 07 PDFShwe Maw KunPas encore d'évaluation
- Tutorial NotesDocument4 pagesTutorial Notesapi-431813813Pas encore d'évaluation
- BadmintonDocument3 pagesBadmintonjerwin dacumosPas encore d'évaluation
- Minutes MeetingDocument5 pagesMinutes MeetingNa'im Yaacob En-whyPas encore d'évaluation
- KD 3.7 Recount TextDocument8 pagesKD 3.7 Recount Textmddspcy lurPas encore d'évaluation
- PDKP Delhi Sports Complex Facilities and Membership FeesDocument5 pagesPDKP Delhi Sports Complex Facilities and Membership FeesDinesh Kumar MeenaPas encore d'évaluation
- Badminton: The History of BadmintonDocument7 pagesBadminton: The History of BadmintonVLyricsPas encore d'évaluation
- Table Tennis: History & DevelopmentDocument11 pagesTable Tennis: History & DevelopmentEurydicePas encore d'évaluation
- Latihan Soal Persiapan UsbnDocument5 pagesLatihan Soal Persiapan Usbnmirah yuliarsianitaPas encore d'évaluation
- Tennis Industry MagazineDocument64 pagesTennis Industry MagazineLiya DavidovPas encore d'évaluation
- Event BrochureDocument16 pagesEvent BrochureCMC PegasusPas encore d'évaluation
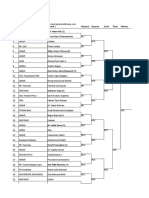
- Draws Unair Open 2019 NewestDocument10 pagesDraws Unair Open 2019 NewestFauzanul AbidinPas encore d'évaluation
- Badminton Lesson PlanDocument7 pagesBadminton Lesson PlanQuinn McKennaPas encore d'évaluation
- VVFDocument14 pagesVVFJohn Remmel RogaPas encore d'évaluation
- UB Badminton Rules: Game Format, Scoring, Service FaultsDocument2 pagesUB Badminton Rules: Game Format, Scoring, Service FaultsManoj RahulPas encore d'évaluation
- Analysis of jumping smash technique in badminton gamesDocument4 pagesAnalysis of jumping smash technique in badminton gamesAsy LimPas encore d'évaluation
- Types of table tennis shots under 40 charactersDocument4 pagesTypes of table tennis shots under 40 charactersjr_rudolfPas encore d'évaluation
- Reaction Time Badminton PlayersDocument9 pagesReaction Time Badminton PlayersRaul ValldecabresPas encore d'évaluation