Vous aimerez peut-être aussi
- Fluid GuidelinesDocument8 pagesFluid GuidelinesAya SalahPas encore d'évaluation
- Fluid and Electrolyte BalanceDocument9 pagesFluid and Electrolyte Balanceamoody95Pas encore d'évaluation
- DehydrationDocument10 pagesDehydrationAbdelrahman M. AlnweiriPas encore d'évaluation
- Pediatric Fluid Therapy GuideDocument27 pagesPediatric Fluid Therapy GuideNanda Cendikia100% (1)
- Fluids and Electrolytes: Rafael Alphonso Pintacasi Class 2016Document32 pagesFluids and Electrolytes: Rafael Alphonso Pintacasi Class 2016Ponchoi PintacasiPas encore d'évaluation
- The I.V Fluids Are Manly Two TypesDocument5 pagesThe I.V Fluids Are Manly Two TypesAbdallah Essam Al-ZireeniPas encore d'évaluation
- PEDIATRIC FLUIDSDocument42 pagesPEDIATRIC FLUIDSSholehuddin MunajjidPas encore d'évaluation
- Pedia Alhamdollilah FluidsDocument80 pagesPedia Alhamdollilah FluidsArwyn AncogPas encore d'évaluation
- Fluids and Electrolytes: Department of Family & Community MedicineDocument40 pagesFluids and Electrolytes: Department of Family & Community MedicineNoornihuma AsharPas encore d'évaluation
- 1 FluidsDocument17 pages1 FluidsMae CalunsagPas encore d'évaluation
- Fluid TherapyDocument27 pagesFluid TherapyRashed ShatnawiPas encore d'évaluation
- Fluid ManagementDocument10 pagesFluid ManagementdradaadPas encore d'évaluation
- Fluid - Electrolyte Imbalance 2012-InedDocument45 pagesFluid - Electrolyte Imbalance 2012-InedmiamuhpianPas encore d'évaluation
- Fluid & Electrolyte Balance: PresentedDocument30 pagesFluid & Electrolyte Balance: PresentedFathimathPas encore d'évaluation
- Intravenous Fluid Therapy: Michael OrnesDocument27 pagesIntravenous Fluid Therapy: Michael OrnesOkto Mara Fandi HarahapPas encore d'évaluation
- IV Fluids: Understanding Daily Requirements and ComplicationsDocument17 pagesIV Fluids: Understanding Daily Requirements and ComplicationsBima BaikuniPas encore d'évaluation
- New Fluid and Electrolytes Therapy Toyinoriginali2againDocument55 pagesNew Fluid and Electrolytes Therapy Toyinoriginali2againt.baby100% (1)
- Fluid and Electrolytes.3Document43 pagesFluid and Electrolytes.3Medic PediatruPas encore d'évaluation
- Types of Fluids and IV Fluid CalculationsDocument3 pagesTypes of Fluids and IV Fluid CalculationsPebblesPas encore d'évaluation
- IV Fluid Management: DR Andrew Stein Consultant Nephrologist, UHCWDocument37 pagesIV Fluid Management: DR Andrew Stein Consultant Nephrologist, UHCWJosh BurkePas encore d'évaluation
- Fluid Electrolyte NutritionDocument40 pagesFluid Electrolyte NutritionStrept PneumoniaPas encore d'évaluation
- Ivfluidtherapytypesindicationsdosescalculation 130123090523 Phpapp01Document68 pagesIvfluidtherapytypesindicationsdosescalculation 130123090523 Phpapp01rainPas encore d'évaluation
- Parenteral Fluid TherapyDocument5 pagesParenteral Fluid TherapyAbdalrahman KhalilPas encore d'évaluation
- IV Infusion SolutionDocument8 pagesIV Infusion SolutionmohammedPas encore d'évaluation
- 1.1a Fluid Management 6th Seminar GRP AaDocument40 pages1.1a Fluid Management 6th Seminar GRP AahalearnPas encore d'évaluation
- IV FluidDocument49 pagesIV Fluidibrahimadnan040Pas encore d'évaluation
- Principles+ +LU6Document35 pagesPrinciples+ +LU6Alvin Ray JuanPas encore d'évaluation
- Guidance For Intravenous Fluid and Electrolyte Prescription in AdultsDocument8 pagesGuidance For Intravenous Fluid and Electrolyte Prescription in AdultsfrakturhepatikaPas encore d'évaluation
- Intravenous Fluid Therapy For 2nd Year ConceptDocument83 pagesIntravenous Fluid Therapy For 2nd Year ConceptMay Chelle ErazoPas encore d'évaluation
- Intravenous Fluid Therapy GuideDocument68 pagesIntravenous Fluid Therapy GuideMourian AmanPas encore d'évaluation
- Body FluidDocument37 pagesBody FluidBir Mohammad SonetPas encore d'évaluation
- Hypernatremic DehydrationDocument3 pagesHypernatremic DehydrationVandanaPas encore d'évaluation
- Clinical PediatricDocument214 pagesClinical PediatricRogerPas encore d'évaluation
- Keeping Fluids and Electrolytes in BalanceDocument9 pagesKeeping Fluids and Electrolytes in BalanceRonello Cyrus FabulaPas encore d'évaluation
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Iv Fluid Therapy in ChildrenDocument12 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Iv Fluid Therapy in ChildrenSREEDEVI T SURESH0% (1)
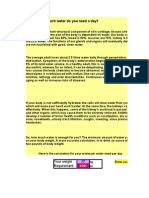
- How Much Water Do You Need A Day?: Your Weight RequirementDocument54 pagesHow Much Water Do You Need A Day?: Your Weight RequirementSiene Pamilar BuenoPas encore d'évaluation
- Hemodialysis: Diffusion and Ultrafiltration: Ramin SamDocument17 pagesHemodialysis: Diffusion and Ultrafiltration: Ramin SamEvelina Navi BraginskiyPas encore d'évaluation
- Fluids and ElectrolytesDocument70 pagesFluids and ElectrolytesCesar MellaPas encore d'évaluation
- Fluids Therapy: Name: Oktavia Sulistiana NIM: G1A214058 Adviser: Dr. Sulistyowati, SP - AnDocument21 pagesFluids Therapy: Name: Oktavia Sulistiana NIM: G1A214058 Adviser: Dr. Sulistyowati, SP - AnoctaviasulistyaPas encore d'évaluation
- Quick Reference Guideline For IV Fluid and Electrolyte Prescribing in AdultsDocument5 pagesQuick Reference Guideline For IV Fluid and Electrolyte Prescribing in AdultsKrishna RajakumarPas encore d'évaluation
- DKA Protocol TGDocument11 pagesDKA Protocol TGabelPas encore d'évaluation
- Maintenance & Replacement Fluid Therapy: Moderated by DR - Madhuri EngadeDocument43 pagesMaintenance & Replacement Fluid Therapy: Moderated by DR - Madhuri EngadeTonny ChenPas encore d'évaluation
- Kidney Regulation of Osmolarity - How the Kidneys Control Salt and Water LevelsDocument4 pagesKidney Regulation of Osmolarity - How the Kidneys Control Salt and Water LevelsYoyo WuPas encore d'évaluation
- Presentation PaedsDocument22 pagesPresentation Paedsosita onajitePas encore d'évaluation
- Diarrhea and DehydrationDocument12 pagesDiarrhea and DehydrationnikprovPas encore d'évaluation
- IvfDocument16 pagesIvfJohnRev Fundal Lopez LorenzoPas encore d'évaluation
- Fluid Management in Pediatrics: Presentor - Dr. Payal Nikose Guide - Dr. Anju AshokanDocument31 pagesFluid Management in Pediatrics: Presentor - Dr. Payal Nikose Guide - Dr. Anju Ashokanvaishnavi kalePas encore d'évaluation
- Fluid Calculation For Iv InfusionDocument8 pagesFluid Calculation For Iv InfusionAsma SaleemPas encore d'évaluation
- Fluid Management For The Pediatric Surgical Patient POWERPOINTDocument34 pagesFluid Management For The Pediatric Surgical Patient POWERPOINTDipta Anggara100% (2)
- HyponatremiaDocument42 pagesHyponatremiaAbdu Raheem100% (1)
- Fluid Management in PediatricsDocument3 pagesFluid Management in PediatricsZiyadPas encore d'évaluation
- Untitled DocumentDocument6 pagesUntitled Documentانس ابوهيبةPas encore d'évaluation
- Pediatric Sodium GuidelineDocument6 pagesPediatric Sodium GuidelineNisa Fithria LathifahPas encore d'évaluation
- Fluids and Electrolytes PediatricsDocument46 pagesFluids and Electrolytes PediatricsShelley PantinoplePas encore d'évaluation
- Hypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandHypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Conn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandConn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- PREPPER'S LONG-TERM SURVIVAL GUIDE: Navigating Challenges and Thriving in Uncertain Times (2023 Guide for Beginners)D'EverandPREPPER'S LONG-TERM SURVIVAL GUIDE: Navigating Challenges and Thriving in Uncertain Times (2023 Guide for Beginners)Pas encore d'évaluation
- Liver TransplantDocument5 pagesLiver TransplantMahmoud SelimPas encore d'évaluation
- Suture TypesDocument2 pagesSuture TypesMahmoud SelimPas encore d'évaluation
- Left Versus Right Lobe Liver Donation: EditorialDocument2 pagesLeft Versus Right Lobe Liver Donation: EditorialMahmoud SelimPas encore d'évaluation
- Print 18Document4 pagesPrint 18Mahmoud SelimPas encore d'évaluation
- How To Start Warfarin TherapyDocument4 pagesHow To Start Warfarin TherapyMahmoud SelimPas encore d'évaluation
- Print 16Document5 pagesPrint 16Mahmoud SelimPas encore d'évaluation
- Factors affecting cost of liver transplantationDocument10 pagesFactors affecting cost of liver transplantationMahmoud SelimPas encore d'évaluation
- How To Start Warfarin TherapyDocument4 pagesHow To Start Warfarin TherapyMahmoud SelimPas encore d'évaluation
- Lung LesionsDocument7 pagesLung LesionsMahmoud SelimPas encore d'évaluation
- Clin Diabetes 2001 Plodkowski 92 5Document4 pagesClin Diabetes 2001 Plodkowski 92 5Mahmoud SelimPas encore d'évaluation
- How To Reverse Low Molecular Weight HeparinDocument2 pagesHow To Reverse Low Molecular Weight HeparinMahmoud SelimPas encore d'évaluation
- Drugs That Effect Wound HealingDocument1 pageDrugs That Effect Wound HealingMahmoud SelimPas encore d'évaluation
- AbstractDocument4 pagesAbstractMahmoud SelimPas encore d'évaluation
- How To Stop Warfarin For Surgery: Low Thromboembolic RiskDocument3 pagesHow To Stop Warfarin For Surgery: Low Thromboembolic RiskMahmoud SelimPas encore d'évaluation
- Clinical Features of Serotonin SyndromeDocument2 pagesClinical Features of Serotonin SyndromeMahmoud SelimPas encore d'évaluation
- Surgical Finals Passing The Clinical PDFDocument40 pagesSurgical Finals Passing The Clinical PDFnetradeep67% (3)
- Pi Is 0168827811611860Document1 pagePi Is 0168827811611860Mahmoud SelimPas encore d'évaluation
- Liver Transplant MedDocument22 pagesLiver Transplant MedMahmoud SelimPas encore d'évaluation
- CefotetanDocument1 pageCefotetanMahmoud SelimPas encore d'évaluation
- Oral Q PDFDocument40 pagesOral Q PDFMahmoud SelimPas encore d'évaluation
- Alchemist - Paulo in ArabicDocument4 pagesAlchemist - Paulo in ArabicMahmoud SelimPas encore d'évaluation
- Nephrol. Dial. Transplant. 2000 Korzets 285 6Document2 pagesNephrol. Dial. Transplant. 2000 Korzets 285 6Mahmoud SelimPas encore d'évaluation
- Plastic Surgery Track II Specific GuidelinesDocument2 pagesPlastic Surgery Track II Specific GuidelinesMahmoud SelimPas encore d'évaluation
- Pi Is 0168827811611860Document1 pagePi Is 0168827811611860Mahmoud SelimPas encore d'évaluation
- ASTS Guidelines for Controlled Donation after Cardiac Death Organ ProcurementDocument8 pagesASTS Guidelines for Controlled Donation after Cardiac Death Organ ProcurementMahmoud SelimPas encore d'évaluation
- Donor Liver Steatosis and Graft Selection For Liver Transplantation: A Short ReviewDocument3 pagesDonor Liver Steatosis and Graft Selection For Liver Transplantation: A Short ReviewMahmoud SelimPas encore d'évaluation
- Overdose and PoisoningDocument4 pagesOverdose and PoisoningMahmoud SelimPas encore d'évaluation
- SURGICAL INSTRUMENTS & SUTURES GUIDEDocument11 pagesSURGICAL INSTRUMENTS & SUTURES GUIDEAhmed Azmy AlgebalyPas encore d'évaluation
- Essential Lists for Intercollegiate MRCS Anaesthetics and ITUDocument18 pagesEssential Lists for Intercollegiate MRCS Anaesthetics and ITUMahmoud Selim100% (1)
- LED Linear Highbay LightingDocument7 pagesLED Linear Highbay LightingMohammed YasarPas encore d'évaluation
- Measurement: Scaling, Reliability, ValidityDocument34 pagesMeasurement: Scaling, Reliability, ValidityFajar Farhan Muhtasir100% (1)
- Triad Over Root Chords Companion PDF 2.1Document18 pagesTriad Over Root Chords Companion PDF 2.1Vlado PetkovskiPas encore d'évaluation
- MetaLINK Info r456Document5 pagesMetaLINK Info r456Milan AntovicPas encore d'évaluation
- Peak Performance 4.3-Inch GPS ManualDocument16 pagesPeak Performance 4.3-Inch GPS ManualmcneelydPas encore d'évaluation
- Useful XFOIL Command ListDocument6 pagesUseful XFOIL Command ListHariharan RamanathanPas encore d'évaluation
- Equipment DetailsDocument10 pagesEquipment Detailsimranjani.skPas encore d'évaluation
- Biophoton Light TherapyDocument1 pageBiophoton Light TherapyVíctor ValdezPas encore d'évaluation
- Certificate: Shear MachineDocument3 pagesCertificate: Shear MachinegilbertoPas encore d'évaluation
- Indigenous Microorganisms Production and The Effect On Composting ProcessDocument5 pagesIndigenous Microorganisms Production and The Effect On Composting ProcessAldrin Baquilid FernandezPas encore d'évaluation
- (PPT) Design of A Low-Power Asynchronous SAR ADC in 45 NM CMOS TechnologyDocument42 pages(PPT) Design of A Low-Power Asynchronous SAR ADC in 45 NM CMOS TechnologyMurod KurbanovPas encore d'évaluation
- As Statistics Mechanics 1Document240 pagesAs Statistics Mechanics 1claire zhouPas encore d'évaluation
- Development and Validation of UV Spectrophotometric Method For The Estimation of Curcumin in Bulk Drug and Pharmaceutical Dosage FormsDocument6 pagesDevelopment and Validation of UV Spectrophotometric Method For The Estimation of Curcumin in Bulk Drug and Pharmaceutical Dosage FormswiracanaPas encore d'évaluation
- Petroleum GeomechanicsDocument35 pagesPetroleum GeomechanicsAnonymous y6UMzakPW100% (1)
- Reed - Camion - XT39R4 - 1003 - Technical Manual - Panel de Control PDFDocument293 pagesReed - Camion - XT39R4 - 1003 - Technical Manual - Panel de Control PDFLuisEduardoHerreraCamargo100% (1)
- Image ReconstructionDocument28 pagesImage ReconstructionRahul PaulPas encore d'évaluation
- CB Climbing Bracket PERIDocument52 pagesCB Climbing Bracket PERINathan FryerPas encore d'évaluation
- Water Quality Study of Kallai RiverDocument43 pagesWater Quality Study of Kallai Riverpratheesh thekedanPas encore d'évaluation
- 7-3 IP Board Part (SMPS Part) : 7 Block DiagramsDocument8 pages7-3 IP Board Part (SMPS Part) : 7 Block DiagramsSonu KumarPas encore d'évaluation
- Operations Management and Decision MakingDocument55 pagesOperations Management and Decision MakingAnkit SinghPas encore d'évaluation
- Section 3 - Vibration MeasurementDocument24 pagesSection 3 - Vibration MeasurementAbbas AkbarPas encore d'évaluation
- DMTH505 Measure Theorey and Functional Analysis PDFDocument349 pagesDMTH505 Measure Theorey and Functional Analysis PDFJahir Uddin LaskarPas encore d'évaluation
- M.SC - Physics 3rd Sem FinalDocument12 pagesM.SC - Physics 3rd Sem FinalKhileswar ChandiPas encore d'évaluation
- Priority Academic Student Skills Mathematics Grades 1-5Document44 pagesPriority Academic Student Skills Mathematics Grades 1-5faithinhim7515Pas encore d'évaluation
- C34 January 2014 (IAL)Document44 pagesC34 January 2014 (IAL)SandyDavidPas encore d'évaluation
- Mark SchemeDocument12 pagesMark SchemeNdanji SiamePas encore d'évaluation
- Theory of Financial Decision Making PDFDocument392 pagesTheory of Financial Decision Making PDFEmmanuel K'pkorPas encore d'évaluation
- POWER Nav1 - MIDTERM - Topic 1 & 2Document31 pagesPOWER Nav1 - MIDTERM - Topic 1 & 2CLIJOHN PABLO FORD100% (1)
- 978402applied Math Test Paper - Xi Set 2 - Sem 2Document4 pages978402applied Math Test Paper - Xi Set 2 - Sem 2MehulPas encore d'évaluation
- Clinical Microscopy ReviewerDocument31 pagesClinical Microscopy ReviewerbokbokbokPas encore d'évaluation