Vous aimerez peut-être aussi
- Step-By-Step Instructions On The: Straumann TibrushDocument4 pagesStep-By-Step Instructions On The: Straumann Tibrushadambear213Pas encore d'évaluation
- JadaDocument14 pagesJadaadambear213Pas encore d'évaluation
- Malpractice and Perio DiseaseDocument4 pagesMalpractice and Perio Diseaseadambear213Pas encore d'évaluation
- 27Document7 pages27adambear213Pas encore d'évaluation
- Keratinized Mucosa Around Dental ImplantsDocument2 pagesKeratinized Mucosa Around Dental Implantsadambear213Pas encore d'évaluation
- Greenstein Et Tarnow 2006ddDocument11 pagesGreenstein Et Tarnow 2006ddAnup Lal RajbahakPas encore d'évaluation
- Periodontal Dictates For Esthetic Ceramometal Crowns: R - Sheldon Stein, DMDDocument11 pagesPeriodontal Dictates For Esthetic Ceramometal Crowns: R - Sheldon Stein, DMDadambear213Pas encore d'évaluation
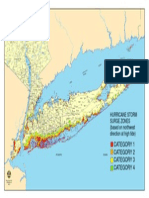
- Nys Storm Surge ZonesDocument1 pageNys Storm Surge Zonesadambear213Pas encore d'évaluation
- Jop 1974 45 3 151Document4 pagesJop 1974 45 3 151adambear213Pas encore d'évaluation
- CDC - Half of American Adults Have Periodontal Disease - PerioDocument3 pagesCDC - Half of American Adults Have Periodontal Disease - Perioadambear213Pas encore d'évaluation
- Dental Office Marketing PlanDocument20 pagesDental Office Marketing PlanPalo Alto Software100% (10)
- Sterile Healing Solutions FOFDocument2 pagesSterile Healing Solutions FOFadambear213Pas encore d'évaluation
- TISPDocument14 pagesTISPadambear213100% (1)
- Ideas Academy Reports: and InnovationsDocument9 pagesIdeas Academy Reports: and Innovationsadambear213Pas encore d'évaluation
- J 1600-0757 1997 tb00094 XDocument21 pagesJ 1600-0757 1997 tb00094 Xadambear213Pas encore d'évaluation
- Average Tooth MeasurmentsDocument1 pageAverage Tooth Measurmentsadambear213Pas encore d'évaluation
- ArticleDocument7 pagesArticleadambear213Pas encore d'évaluation
- REVISED ASSIGNMENTS Biology and Pathology of The PeriodontiumDocument2 pagesREVISED ASSIGNMENTS Biology and Pathology of The Periodontiumadambear213Pas encore d'évaluation
- 16Document9 pages16adambear213Pas encore d'évaluation
- WhatsNew E OldDocument25 pagesWhatsNew E Oldadambear213Pas encore d'évaluation
- WhatsNew EDocument37 pagesWhatsNew Eadambear213Pas encore d'évaluation
- Suture Surg Gut Chrom Bge FS2 4Document1 pageSuture Surg Gut Chrom Bge FS2 4adambear213Pas encore d'évaluation
- Map ArenaDocument1 pageMap Arenaadambear213Pas encore d'évaluation
- IBR Application CDocument12 pagesIBR Application CChris HudginsPas encore d'évaluation
- Sterile Healing Solutions FOFDocument2 pagesSterile Healing Solutions FOFadambear213Pas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- DDR PrimeDocument4 pagesDDR PrimeNona AlyPas encore d'évaluation
- Carboprost Drug StudyDocument3 pagesCarboprost Drug StudyAjay SupanPas encore d'évaluation
- The Amazing Science of AuriculotherapyDocument26 pagesThe Amazing Science of AuriculotherapyNatura888100% (13)
- Learning Module in NCM 114Document28 pagesLearning Module in NCM 114JIMENEZ, TRISHA MARIE D.Pas encore d'évaluation
- Format Pencatatan Hasil Pelayanan Vaksinasi Manual Pusk Fasyankes PosDocument48 pagesFormat Pencatatan Hasil Pelayanan Vaksinasi Manual Pusk Fasyankes PosluveliaPas encore d'évaluation
- Ob Nursing Care Plan For Maternal Database Maternal and NewbornDocument2 pagesOb Nursing Care Plan For Maternal Database Maternal and Newbornapi-403051801Pas encore d'évaluation
- NURS FPX 5005 Assessment 1 Protecting Human Research ParticipantsDocument4 pagesNURS FPX 5005 Assessment 1 Protecting Human Research ParticipantsEmma WatsonPas encore d'évaluation
- Healthcare Disinfection and Sterilization GuideDocument8 pagesHealthcare Disinfection and Sterilization GuideAyu AndrianiPas encore d'évaluation
- Danielle Nesbit: Work ExperienceDocument4 pagesDanielle Nesbit: Work ExperienceNav SethPas encore d'évaluation
- Drugs in Europe-EUDocument43 pagesDrugs in Europe-EUDenisa Elena APas encore d'évaluation
- JensenDocument19 pagesJensencarol colmenaresPas encore d'évaluation
- MTLB Debate PRODocument3 pagesMTLB Debate PRORHODA MAE CAPUTOLPas encore d'évaluation
- Series Screenwriter Portfolio by SlidesgoDocument24 pagesSeries Screenwriter Portfolio by SlidesgoYeddah Gwyneth TiuPas encore d'évaluation
- Managing Health For Field Operations in Oil and Gas ActivitiesDocument44 pagesManaging Health For Field Operations in Oil and Gas ActivitiesHaleemUrRashidBangashPas encore d'évaluation
- 12 Tips For Bedside TeachingDocument4 pages12 Tips For Bedside Teachingbayu100% (1)
- A Cross Sectional Survey On Sleep Quality, Mental Health, and Academic Performance Among Medical Student in Saudia ArabiaDocument5 pagesA Cross Sectional Survey On Sleep Quality, Mental Health, and Academic Performance Among Medical Student in Saudia ArabiaReynaldy Anggara SaputraPas encore d'évaluation
- DEFTACDocument8 pagesDEFTACPendon Maria Mikhaela PPas encore d'évaluation
- Gastro Inter It IsDocument3 pagesGastro Inter It IsDhea Imas WijayantiPas encore d'évaluation
- Simulation Program For Clinical Performance Improvement: Improving Clinical Care and Patient Safety Through SimulationDocument11 pagesSimulation Program For Clinical Performance Improvement: Improving Clinical Care and Patient Safety Through SimulationiloilocityPas encore d'évaluation
- Incidence and Factors Related To Flare-Ups in A Graduate Endodontic ProgrammeDocument7 pagesIncidence and Factors Related To Flare-Ups in A Graduate Endodontic ProgrammeRose FlawerPas encore d'évaluation
- Second Degree Burn Injury in A CowDocument2 pagesSecond Degree Burn Injury in A CowvetarifPas encore d'évaluation
- Salvia, DivornumDocument1 pageSalvia, Divornumeab7686Pas encore d'évaluation
- Case Study Bronchial Asthma-1Document13 pagesCase Study Bronchial Asthma-1Krishna Krishii AolPas encore d'évaluation
- Student Nurses' Seizure CareDocument2 pagesStudent Nurses' Seizure CareIanne Najial100% (3)
- ResearchDocument3 pagesResearchAhtisham NadeemPas encore d'évaluation
- Bum Run GradDocument10 pagesBum Run GradsabyasachiPas encore d'évaluation
- Kanker PayudaraDocument60 pagesKanker PayudaranoviPas encore d'évaluation
- BeWell Assignment 2 W22Document8 pagesBeWell Assignment 2 W22Christian SNPas encore d'évaluation
- Model Question Papers AnmDocument8 pagesModel Question Papers AnmAbhijit Sanjeev77% (13)
- Gastrostomy FeedingDocument8 pagesGastrostomy FeedingToka HessenPas encore d'évaluation