Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Facs ProtocolDocument7 pagesFacs ProtocolmisterxPas encore d'évaluation
- BT 2019Document13 pagesBT 2019biotech_vidhyaPas encore d'évaluation
- Stripping For ReprobingDocument2 pagesStripping For ReprobingStella SalvatorePas encore d'évaluation
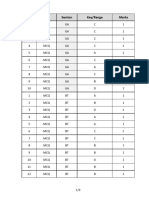
- Q.No. Type Section Key/Range MarksDocument3 pagesQ.No. Type Section Key/Range Marksbiotech_vidhyaPas encore d'évaluation
- Stripping For ReprobingDocument2 pagesStripping For ReprobingStella SalvatorePas encore d'évaluation
- Polymerase Chain Reaction (PCR)Document3 pagesPolymerase Chain Reaction (PCR)biotech_vidhyaPas encore d'évaluation
- Brad FordDocument12 pagesBrad FordQi ChaoPas encore d'évaluation
- SDS PageDocument2 pagesSDS Pagebiotech_vidhyaPas encore d'évaluation
- Buffer Preparation Guide for DNA/Protein Work (Shi LabDocument6 pagesBuffer Preparation Guide for DNA/Protein Work (Shi Labbiotech_vidhyaPas encore d'évaluation
- Troubleshooting SDS-PAGE 1Document3 pagesTroubleshooting SDS-PAGE 1biotech_vidhyaPas encore d'évaluation
- Polymerasen GuideDocument16 pagesPolymerasen Guidebiotech_vidhyaPas encore d'évaluation
- Components Reaction MixtureDocument3 pagesComponents Reaction Mixturebiotech_vidhyaPas encore d'évaluation
- Buffer Preparation Guide for DNA/Protein Work (Shi LabDocument6 pagesBuffer Preparation Guide for DNA/Protein Work (Shi Labbiotech_vidhyaPas encore d'évaluation
- TNPSC Group 1 Prelim Book List PDFDocument2 pagesTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaPas encore d'évaluation
- Whole Cell ExtractDocument1 pageWhole Cell Extractbiotech_vidhyaPas encore d'évaluation
- TNPSC Group 1 Prelim Book List PDFDocument2 pagesTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaPas encore d'évaluation
- Befcv List PDFDocument22 pagesBefcv List PDFbiotech_vidhyaPas encore d'évaluation
- Nuclear ExtractsDocument2 pagesNuclear Extractsbiotech_vidhyaPas encore d'évaluation
- Qpaper PondyDocument21 pagesQpaper Pondybiotech_vidhyaPas encore d'évaluation
- Ies 17 Set A Me Q ADocument67 pagesIes 17 Set A Me Q Abiotech_vidhyaPas encore d'évaluation
- TNPSC Group 1 Prelim Book List PDFDocument2 pagesTNPSC Group 1 Prelim Book List PDFbiotech_vidhyaPas encore d'évaluation
- A.E. (Mechanical Engineering I) 2007Document24 pagesA.E. (Mechanical Engineering I) 2007Mukesh KumarPas encore d'évaluation
- Qpaper PondyDocument21 pagesQpaper Pondybiotech_vidhyaPas encore d'évaluation
- ESE 2017 Mechanical Engineering Prelims Exam Detailed SolutionDocument52 pagesESE 2017 Mechanical Engineering Prelims Exam Detailed SolutionpataPas encore d'évaluation
- Img Word-To PDFDocument3 pagesImg Word-To PDFbiotech_vidhyaPas encore d'évaluation
- Mechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010Document20 pagesMechanical Engineering Code No. 14: Combined Competitive (Preliminary) Examination, 2010biotech_vidhyaPas encore d'évaluation
- TDC 41597 A (Mechanical Engg.) - 2012Document20 pagesTDC 41597 A (Mechanical Engg.) - 2012biotech_vidhyaPas encore d'évaluation
- Recruitment RulesDocument5 pagesRecruitment Rulesbiotech_vidhyaPas encore d'évaluation
- Part and Mold Design GuideDocument170 pagesPart and Mold Design GuideminhtintinPas encore d'évaluation
- 1 TolerancesDocument1 page1 Tolerancesbiotech_vidhyaPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Phagocytosis Assay Kit (Igg Fitc) : Item No. 500290Document9 pagesPhagocytosis Assay Kit (Igg Fitc) : Item No. 500290drfiatPas encore d'évaluation
- Ecg Quick Guide PDFDocument7 pagesEcg Quick Guide PDFansarijavedPas encore d'évaluation
- Master Tong-Style Acupuncturist Interview Part 1Document4 pagesMaster Tong-Style Acupuncturist Interview Part 1Anonymous uMnup2r100% (1)
- Final Benzodiazepine Guidelines Version 23 1495194854Document18 pagesFinal Benzodiazepine Guidelines Version 23 1495194854Kru PrimePas encore d'évaluation
- Congenital Talipes Equino-Varus (Congenital Clubfoot) : Prof. Sohail Iqbal Sheikh Hod/Orthopaedics Iimct/PrhDocument66 pagesCongenital Talipes Equino-Varus (Congenital Clubfoot) : Prof. Sohail Iqbal Sheikh Hod/Orthopaedics Iimct/Prhawaisjinnah100% (1)
- Petridou, Thumiger-Homo Patiens - Approaches To The Patient in The Ancient World (SAM 45)Document555 pagesPetridou, Thumiger-Homo Patiens - Approaches To The Patient in The Ancient World (SAM 45)jeremy_luckas100% (1)
- Tugas B.inggrisDocument14 pagesTugas B.inggrisLove.u. TooPas encore d'évaluation
- Aman Foundation Internship Application FormDocument4 pagesAman Foundation Internship Application Formabdullahnisar92Pas encore d'évaluation
- CH 25 Respiration Study GuideDocument2 pagesCH 25 Respiration Study Guide99646qbkdwPas encore d'évaluation
- Hospital Job DescriptionsDocument48 pagesHospital Job DescriptionsLoresita Amoranto Rebong RNPas encore d'évaluation
- Thyroid Gland AnatomyDocument11 pagesThyroid Gland AnatomyRem AlfelorPas encore d'évaluation
- Reading Sub-Test: Answer Key - Part ADocument23 pagesReading Sub-Test: Answer Key - Part AAlwin BrightPas encore d'évaluation
- 01 1 PDFDocument8 pages01 1 PDFpravikumar1989Pas encore d'évaluation
- Maximum Marks: 100Document35 pagesMaximum Marks: 100Yu HoyanPas encore d'évaluation
- Orthovoltage Vs MegavoltageDocument7 pagesOrthovoltage Vs MegavoltageEmmanuel Cuevas MisPas encore d'évaluation
- DiaDENS-Cardio Operations ManualDocument37 pagesDiaDENS-Cardio Operations Manualgetdenas100% (4)
- Pahs Mbbs Information BookletDocument18 pagesPahs Mbbs Information BookletKishor BajgainPas encore d'évaluation
- Mini Question Bank - Vety Sci - For Students PDFDocument106 pagesMini Question Bank - Vety Sci - For Students PDFRakesh Prajapati100% (3)
- Synthesis of Novel Amino Acid Derivative of 7-AVCADocument4 pagesSynthesis of Novel Amino Acid Derivative of 7-AVCAIOSRjournal0% (1)
- Treatment Head LiceDocument26 pagesTreatment Head LiceCherry Amor Betita MadronaPas encore d'évaluation
- Treponema Pallidum: Human PathogensDocument27 pagesTreponema Pallidum: Human PathogensGeorgeNecoarăPas encore d'évaluation
- Human Papillomavirus (HPV) Test and PAP Smear As Predictors of Outcome in Conservatively Treated Adenocarcinoma in Situ (AIS) of The Uterine CervixDocument7 pagesHuman Papillomavirus (HPV) Test and PAP Smear As Predictors of Outcome in Conservatively Treated Adenocarcinoma in Situ (AIS) of The Uterine CervixodivarPas encore d'évaluation
- Herb II-5-Herbs That Tonify Qi & BloodDocument51 pagesHerb II-5-Herbs That Tonify Qi & BloodEdison halimPas encore d'évaluation
- Assessment Diagnosis Planning Interventions Rationale Evaluation Subjective: "Maglisod Man Kog Short Term: Independent: - Establish RapportDocument3 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Subjective: "Maglisod Man Kog Short Term: Independent: - Establish RapportSergi Lee OratePas encore d'évaluation
- Procedimento Implante AmbicorDocument12 pagesProcedimento Implante Ambicorapi-3762376Pas encore d'évaluation
- Acute Care TestingDocument222 pagesAcute Care TestingAdel ChaabanePas encore d'évaluation
- 53 Vol. 6 Issue 7 IJPSR 2015 RA 4953Document9 pages53 Vol. 6 Issue 7 IJPSR 2015 RA 4953Dina AyupnPas encore d'évaluation
- Pott's DiseaseDocument8 pagesPott's DiseaseBij HilarioPas encore d'évaluation
- Q4 Health 6 Week3Document4 pagesQ4 Health 6 Week3Ethelyn Joy FarquerabaoPas encore d'évaluation
- Clonus: Definition, Mechanism, Treatment: ReviewDocument8 pagesClonus: Definition, Mechanism, Treatment: ReviewLuqmanul HakimPas encore d'évaluation