Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Dear Ni Putu Pristi, Dear Dr. Risca Rini,: Andreas Asked.... I Said Yes. Andreas Asked.... I Said YesDocument1 pageDear Ni Putu Pristi, Dear Dr. Risca Rini,: Andreas Asked.... I Said Yes. Andreas Asked.... I Said YesRessy HastoprajaPas encore d'évaluation
- Dear Dr. Meilinda, Dear Debora,: Andreas Asked.... I Said Yes. Andreas Asked.... I Said YesDocument1 pageDear Dr. Meilinda, Dear Debora,: Andreas Asked.... I Said Yes. Andreas Asked.... I Said YesRessy HastoprajaPas encore d'évaluation
- J. Antimicrob. Chemother. 2014 Kalita Jac Dku103Document6 pagesJ. Antimicrob. Chemother. 2014 Kalita Jac Dku103Ressy HastoprajaPas encore d'évaluation
- Daftar Pustaka: Akhir. Jakarta: Prestasi Pusaka.2008Document1 pageDaftar Pustaka: Akhir. Jakarta: Prestasi Pusaka.2008Ressy HastoprajaPas encore d'évaluation
- Predictors of Stroke in Patient With Meningitis TB and Its Effect and Outcome QMJ 2010Document8 pagesPredictors of Stroke in Patient With Meningitis TB and Its Effect and Outcome QMJ 2010Ressy HastoprajaPas encore d'évaluation
- Ampullary CA Associated With An Annular PancreasDocument5 pagesAmpullary CA Associated With An Annular PancreasRessy HastoprajaPas encore d'évaluation
- Print Morpot 8 MaretDocument3 pagesPrint Morpot 8 MaretRessy HastoprajaPas encore d'évaluation
- Morpot Dispepsia + ISKDocument12 pagesMorpot Dispepsia + ISKRessy HastoprajaPas encore d'évaluation
- Meljo Laporan Ok Kuretase DR MP 4 September 2015Document2 pagesMeljo Laporan Ok Kuretase DR MP 4 September 2015Ressy HastoprajaPas encore d'évaluation
- Multi Drug Resistant (MDR) Tuberculous Meningitis With HydrosefalusDocument4 pagesMulti Drug Resistant (MDR) Tuberculous Meningitis With HydrosefalusRessy HastoprajaPas encore d'évaluation
- Morpot Dispepsia + ISKDocument12 pagesMorpot Dispepsia + ISKRessy HastoprajaPas encore d'évaluation
- Morning Report Ny RamsudarDocument12 pagesMorning Report Ny RamsudarRessy HastoprajaPas encore d'évaluation
- 16710Document5 pages16710Ressy HastoprajaPas encore d'évaluation
- BFT VanriemsdijkDocument2 pagesBFT VanriemsdijkRessy HastoprajaPas encore d'évaluation
- Pi Is 0002937813009927Document7 pagesPi Is 0002937813009927Ressy HastoprajaPas encore d'évaluation
- Neuraxial ProceduresDocument2 pagesNeuraxial ProceduresRessy HastoprajaPas encore d'évaluation
- Cover Refarat CA NasofaringDocument1 pageCover Refarat CA NasofaringRessy HastoprajaPas encore d'évaluation
- Prolonged Pregnancy Induction of Labor And.9Document5 pagesProlonged Pregnancy Induction of Labor And.9Ressy HastoprajaPas encore d'évaluation
- Cover Referat Carpal Tunnel Syndrome Evan FixDocument1 pageCover Referat Carpal Tunnel Syndrome Evan FixRessy HastoprajaPas encore d'évaluation
- Mutia-Logistik, Anggaran IFOODEXDocument9 pagesMutia-Logistik, Anggaran IFOODEXRessy HastoprajaPas encore d'évaluation
- Br. J. Anaesth. 2011 Horlocker I96 I106Document11 pagesBr. J. Anaesth. 2011 Horlocker I96 I106Ressy HastoprajaPas encore d'évaluation
- Cover Referat Carpal Tunnel Syndrome Evan FixDocument1 pageCover Referat Carpal Tunnel Syndrome Evan FixRessy HastoprajaPas encore d'évaluation
- Morning Report GE Da BestttttttDocument12 pagesMorning Report GE Da BestttttttRessy HastoprajaPas encore d'évaluation
- Cover Referat Carpal Tunnel Syndrome Evan FixDocument1 pageCover Referat Carpal Tunnel Syndrome Evan FixRessy HastoprajaPas encore d'évaluation
- ImpetigoDocument24 pagesImpetigoIvan Sitohang100% (2)
- Cover Referat Carpal Tunnel Syndrome Evan FixDocument1 pageCover Referat Carpal Tunnel Syndrome Evan FixRessy HastoprajaPas encore d'évaluation
- ImpetigoDocument24 pagesImpetigoIvan Sitohang100% (2)
- Pathophysiology of HypertensionDocument14 pagesPathophysiology of HypertensionRessy HastoprajaPas encore d'évaluation
- KomodoDocument6 pagesKomodoRessy HastoprajaPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Presentationpp 31 40 12 15Document14 pagesPresentationpp 31 40 12 15hasanmiya rindePas encore d'évaluation
- Anti Inflamasi Dan ANALGETIK (Anti Nociceptive)Document30 pagesAnti Inflamasi Dan ANALGETIK (Anti Nociceptive)SEPTIANA SAPUTRIPas encore d'évaluation
- Tacrolimus TopicalDocument5 pagesTacrolimus TopicalSetyabella Ika PutriPas encore d'évaluation
- Annex 8: Proposal To Waive in Vivo Bioequivalence Requirements For WHO Model List of EssentialDocument49 pagesAnnex 8: Proposal To Waive in Vivo Bioequivalence Requirements For WHO Model List of Essentialrnd_holiPas encore d'évaluation
- Lesson 1 Prescription and Medication OrderDocument30 pagesLesson 1 Prescription and Medication OrderAngelica GomezPas encore d'évaluation
- Statins Side Effects - Pain, Inflammation, and MoreDocument6 pagesStatins Side Effects - Pain, Inflammation, and MoreJeff TeePas encore d'évaluation
- LisinoprilDocument1 pageLisinoprilKatie McPeekPas encore d'évaluation
- PRICELIST JANUARI 2022 (AutoRecovered)Document26 pagesPRICELIST JANUARI 2022 (AutoRecovered)taufanmjPas encore d'évaluation
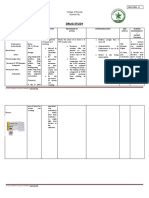
- Drug Study: La Salle UniversityDocument3 pagesDrug Study: La Salle UniversityJb RosillosaPas encore d'évaluation
- Lecture 2 Opoid Analgesics PDFDocument12 pagesLecture 2 Opoid Analgesics PDFAbdelrahman WaelPas encore d'évaluation
- Anti Hypertensive Drugs - DiureticsDocument49 pagesAnti Hypertensive Drugs - DiureticsApurba Sarker Apu100% (1)
- Acil Cantasi Kontrol FormuDocument1 pageAcil Cantasi Kontrol Formuebnem nizamPas encore d'évaluation
- Pharmacology - The Drug Development ProcessDocument3 pagesPharmacology - The Drug Development ProcessCamilogsPas encore d'évaluation
- Class 5Document430 pagesClass 5Subash NeupanePas encore d'évaluation
- Drug SheetDocument3 pagesDrug Sheetavause2Pas encore d'évaluation
- Skeletal Muscle RelaxantsDocument10 pagesSkeletal Muscle RelaxantsJanelle Bondad100% (1)
- Phar LMRDocument5 pagesPhar LMRakshayPas encore d'évaluation
- Guidelines For The Use of Paliperidone Palmitate V2xDocument7 pagesGuidelines For The Use of Paliperidone Palmitate V2xrajeevsonaliPas encore d'évaluation
- Swot GileadDocument9 pagesSwot GileadMutia Poetry MandelaPas encore d'évaluation
- Case Study - Erics Expanding WaistlineDocument6 pagesCase Study - Erics Expanding WaistlineKimberly George-BalgobinPas encore d'évaluation
- Multi-Drug One Step Screen Test Panel (Urine) IFUDocument3 pagesMulti-Drug One Step Screen Test Panel (Urine) IFUIgnacio PerezPas encore d'évaluation
- STOK250921Document36 pagesSTOK250921Martha AdinataPas encore d'évaluation
- Medication: Expected Pharmacological Action Therapeutic UseDocument1 pageMedication: Expected Pharmacological Action Therapeutic UseJeffrey BurdPas encore d'évaluation
- Mometasone FuroatDocument8 pagesMometasone FuroatAnonymous ZrLxxRUr9zPas encore d'évaluation
- Alvin Gabriel L. AltarejosDocument17 pagesAlvin Gabriel L. AltarejosKeanu AlvarezPas encore d'évaluation
- Test Bank For Lehnes Pharmacology For Nursing Care Burchum 9th EditionDocument11 pagesTest Bank For Lehnes Pharmacology For Nursing Care Burchum 9th EditionHenry Horowitz100% (28)
- Cannabis PoisoningDocument24 pagesCannabis PoisoningAkhilaPas encore d'évaluation
- PricelistDocument4 pagesPricelistMAYMART CASABAPas encore d'évaluation
- IV CompatibilityDocument44 pagesIV CompatibilityPhoebe SedantesPas encore d'évaluation
- Cholestyramine (Drug Study)Document2 pagesCholestyramine (Drug Study)Franz.thenurse6888Pas encore d'évaluation