Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Treatment of Menopausal Symptoms With Hormone TherapyDocument17 pagesTreatment of Menopausal Symptoms With Hormone TherapyCésar Vásquez AguilarPas encore d'évaluation
- STROKE - Mimics y DGDocument15 pagesSTROKE - Mimics y DGCésar Vásquez AguilarPas encore d'évaluation
- Electrocardiography: The ECG: A.D. John, MD, Lee A. Fleisher, MDDocument19 pagesElectrocardiography: The ECG: A.D. John, MD, Lee A. Fleisher, MDCésar Vásquez AguilarPas encore d'évaluation
- STROKE - Resumen de Warlow en LancetDocument14 pagesSTROKE - Resumen de Warlow en LancetCésar Vásquez AguilarPas encore d'évaluation
- Epilepsy: P E SmithDocument8 pagesEpilepsy: P E SmithosvaldolarasPas encore d'évaluation
- COMADocument10 pagesCOMAVictorF2Pas encore d'évaluation
- Profilaxis Migraña JNNP Pract Neurol 2007Document11 pagesProfilaxis Migraña JNNP Pract Neurol 2007César Vásquez Aguilar0% (1)
- Viral Encephalitis: A Clinician's Guide: Practical NeurologyDocument19 pagesViral Encephalitis: A Clinician's Guide: Practical NeurologyCésar Vásquez Aguilar100% (1)
- Em - Revision Del Lancet-1Document16 pagesEm - Revision Del Lancet-1César Vásquez AguilarPas encore d'évaluation
- AlzheimerDocument13 pagesAlzheimerleandrolucasvalePas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Illustrated Book of Pediatrics 2ndDocument975 pagesIllustrated Book of Pediatrics 2ndCarla Tapia Norambuena100% (2)
- Management of Fournier GangrenDocument4 pagesManagement of Fournier GangrenArby ShafaraPas encore d'évaluation
- CH 35 Dental Handpieces and Accessories3641Document32 pagesCH 35 Dental Handpieces and Accessories3641Suvasish Suvasish50% (2)
- HemostasisDocument133 pagesHemostasisAishwarya S. Nair100% (6)
- A Survey of Stent Designs PDFDocument11 pagesA Survey of Stent Designs PDFGabriel Lopez BarajasPas encore d'évaluation
- Dekker Surgical Atlas of Pediatric OtolaryngologyDocument865 pagesDekker Surgical Atlas of Pediatric OtolaryngologyDaniel Rajkumar100% (2)
- Dicynone InjectionDocument3 pagesDicynone InjectionAhmed Ebid100% (2)
- Congenital Heart DiseaseDocument10 pagesCongenital Heart DiseaseIca JustitiaPas encore d'évaluation
- MMDSTDocument2 pagesMMDSTBianca MolinaPas encore d'évaluation
- Standard Operating Procedure Manual For Obstetrics and Midwifery ServicesDocument64 pagesStandard Operating Procedure Manual For Obstetrics and Midwifery ServicesTmanoj Praveen75% (4)
- Paediatric NeuroanaesthesiaDocument28 pagesPaediatric Neuroanaesthesiakoolstarone100% (1)
- ProspectusDocument92 pagesProspectusAnwer SaidPas encore d'évaluation
- DM MCHDocument2 pagesDM MCHBhalodiya NirajPas encore d'évaluation
- Dermatology and VenereologyDocument55 pagesDermatology and Venereologykloter1Pas encore d'évaluation
- Does The UNOS Heart Transplant Allocation System Favor Men Over Women?Document9 pagesDoes The UNOS Heart Transplant Allocation System Favor Men Over Women?Thumper KatesPas encore d'évaluation
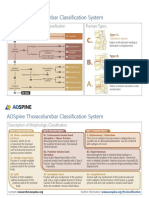
- AOSpine Thoracolumbar Classification System - Pocket CardDocument2 pagesAOSpine Thoracolumbar Classification System - Pocket CardFernanda Ahumada0% (1)
- Bicon Catalog 2012Document68 pagesBicon Catalog 2012Bicon Implant InaPas encore d'évaluation
- Sun Pharma IR PresentationDocument56 pagesSun Pharma IR PresentationAishwarya MauryaPas encore d'évaluation
- The Little Doctor by Juan J. GuerraDocument3 pagesThe Little Doctor by Juan J. GuerraArte Público PressPas encore d'évaluation
- Doctor Su-Kabtas Family PracticeDocument6 pagesDoctor Su-Kabtas Family PracticeSrood TalibPas encore d'évaluation
- A Clinical Study On Oligohydramnios in The ThirdDocument23 pagesA Clinical Study On Oligohydramnios in The ThirdDickyPas encore d'évaluation
- File 925Document26 pagesFile 925SadishPas encore d'évaluation
- Prom 1Document48 pagesProm 1Tesfahun TeklePas encore d'évaluation
- AnatoFisio VestibularDocument17 pagesAnatoFisio VestibularRocío YáñezPas encore d'évaluation
- KPI-Percentage of Day Surgery CasesDocument1 pageKPI-Percentage of Day Surgery Casesangeli punoPas encore d'évaluation
- Bipa Annual Conference Programme 2012Document3 pagesBipa Annual Conference Programme 2012JP RajendranPas encore d'évaluation
- Audio03 AudiometryDocument37 pagesAudio03 AudiometryNafees AnjumPas encore d'évaluation
- Harvey Learner ManualDocument89 pagesHarvey Learner ManualericPas encore d'évaluation
- Apical Extrusion of Debris and Irrigant Using HandDocument25 pagesApical Extrusion of Debris and Irrigant Using HandManva MonishPas encore d'évaluation
- Img 20191231 153040Document1 pageImg 20191231 153040Sajal SarkarPas encore d'évaluation