Vous aimerez peut-être aussi
- For PrintingDocument1 pageFor PrintingHowell YapPas encore d'évaluation
- Opd Meds Jgej PDFDocument4 pagesOpd Meds Jgej PDFKaty SanchezPas encore d'évaluation
- Compiled Case Study-LenovoDocument24 pagesCompiled Case Study-LenovoHowell Yap100% (2)
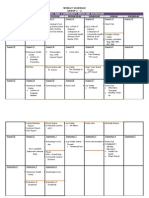
- FM Rotation Weekly Schedule Group C-2Document2 pagesFM Rotation Weekly Schedule Group C-2Howell YapPas encore d'évaluation
- W10 Water, Vitamins & MineralsDocument37 pagesW10 Water, Vitamins & MineralsHowell YapPas encore d'évaluation
- Psychiatric Nursing ReviewDocument16 pagesPsychiatric Nursing Reviewɹǝʍdןnos97% (63)
- CCMH NCPDocument7 pagesCCMH NCPajheihPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Immunologic Mechanisms in AsthmaDocument9 pagesImmunologic Mechanisms in AsthmaKessi VikaneswariPas encore d'évaluation
- Allergic RhinitisDocument30 pagesAllergic RhinitisNoor Al AhmadPas encore d'évaluation
- Histo Trans Lec 3 1 PDFDocument8 pagesHisto Trans Lec 3 1 PDFBreville SagePas encore d'évaluation
- APJAI CPG For Diagnosis & Management of UrticariaDocument11 pagesAPJAI CPG For Diagnosis & Management of UrticariaInternal MedicinePas encore d'évaluation
- R V ChandranDocument3 pagesR V Chandran3701Dhanush NadarPas encore d'évaluation
- Bao (2019), Human Health, Legislative and Socioeconomic Issues Caused by The Fish-Borne Zoonotic Parasite Anisakis Challenges in Risk AssessmentDocument13 pagesBao (2019), Human Health, Legislative and Socioeconomic Issues Caused by The Fish-Borne Zoonotic Parasite Anisakis Challenges in Risk AssessmentCarito ErasoPas encore d'évaluation
- Immunoglobulins: Dr. Pendru RaghunathDocument26 pagesImmunoglobulins: Dr. Pendru RaghunathRupika SyalPas encore d'évaluation
- Cholinergic Urticaria Subtype Classification and Clinical ApproachDocument14 pagesCholinergic Urticaria Subtype Classification and Clinical ApproachKikin RizkynnisaPas encore d'évaluation
- PATHOLOGY Board Exam ANsWERSDocument22 pagesPATHOLOGY Board Exam ANsWERSchristinejoan100% (1)
- HypersensitivityDocument6 pagesHypersensitivitykuldip.biotech100% (1)
- Flare Ups in Endodontics - 1 Etiological FactorsDocument6 pagesFlare Ups in Endodontics - 1 Etiological FactorsdrshravyaPas encore d'évaluation
- Sorted Feedback TopicwiseDocument55 pagesSorted Feedback TopicwiseLokesh BakshiPas encore d'évaluation
- Asthma and COPD - Bashayer & Afrah & EmanDocument6 pagesAsthma and COPD - Bashayer & Afrah & EmanHassan.shehriPas encore d'évaluation
- Air Microflora in Allergic Disorders ofDocument31 pagesAir Microflora in Allergic Disorders ofhrishikesh08100% (1)
- 11BCDocument23 pages11BCMuhammad Qamar NazirPas encore d'évaluation
- Hypersensitivity ReactionDocument36 pagesHypersensitivity ReactionMohana Sundaram100% (1)
- PIIS0091674911015594Document6 pagesPIIS0091674911015594danaagus81Pas encore d'évaluation
- Antibody Structure and FuncionDocument6 pagesAntibody Structure and FuncionMPas encore d'évaluation
- Chronic Spontaneous UrticariaDocument28 pagesChronic Spontaneous UrticariamaryPas encore d'évaluation
- Brain Tumor Epidemiology: Consensus From The Brain Tumor Epidemiology ConsortiumDocument16 pagesBrain Tumor Epidemiology: Consensus From The Brain Tumor Epidemiology ConsortiumscrugnlorPas encore d'évaluation
- Global Atlas of Allergic Rhinitis & Chronic Rhinosinusitis ENT - Atlas - WebDocument442 pagesGlobal Atlas of Allergic Rhinitis & Chronic Rhinosinusitis ENT - Atlas - WebNadiaPas encore d'évaluation
- Morgan Mikhails Clinical Anesthesiology 6th Ed 2018 (2114-2211)Document98 pagesMorgan Mikhails Clinical Anesthesiology 6th Ed 2018 (2114-2211)Wiwik SundariPas encore d'évaluation
- Omalizumab in DermatologyDocument35 pagesOmalizumab in DermatologyDeval MistryPas encore d'évaluation
- Bajwa, 2018 - Atopic Dermatitis in CatsDocument3 pagesBajwa, 2018 - Atopic Dermatitis in CatsFabricio CamargoPas encore d'évaluation
- Basic Bacteriology McqsDocument25 pagesBasic Bacteriology Mcqshassan qureshi100% (1)
- Question Text Question Type PointsDocument25 pagesQuestion Text Question Type PointsMagda Tvildiani100% (1)
- Study Notes Respiratory SystemDocument19 pagesStudy Notes Respiratory SystemAnde Mangkuluhur Azhari ThalibbanPas encore d'évaluation
- Westie Heal The BookDocument177 pagesWestie Heal The BookNemo Westie Ogi IIPas encore d'évaluation
- Canine Atopic DermatitisDocument16 pagesCanine Atopic Dermatitisserbanbogdans536667% (3)
- The Blood: Rubie Maranan-Causaren, MSDocument73 pagesThe Blood: Rubie Maranan-Causaren, MSlady ann jimenez100% (3)