Vous aimerez peut-être aussi
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYD'EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYPas encore d'évaluation
- Dolor Postop, Ligamentos Cruzados, AmbulatorioDocument7 pagesDolor Postop, Ligamentos Cruzados, AmbulatorioChurrunchaPas encore d'évaluation
- JCM 08 02014 v2Document9 pagesJCM 08 02014 v2burhanPas encore d'évaluation
- 0 Aet484Document7 pages0 Aet484UsbahPas encore d'évaluation
- Effect of Pharyngeal Packing During Nasal SurgeryDocument12 pagesEffect of Pharyngeal Packing During Nasal SurgeryRahma R SPas encore d'évaluation
- 1828 1833Document6 pages1828 1833abdulPas encore d'évaluation
- 与扑热息痛联用增效Document5 pages与扑热息痛联用增效zhuangemrysPas encore d'évaluation
- Effects of Propofol Anesthesia Versus SevofluraneDocument33 pagesEffects of Propofol Anesthesia Versus SevofluraneJuwita PratiwiPas encore d'évaluation
- 404 2019 Article 5260Document7 pages404 2019 Article 5260Farida SiggiPas encore d'évaluation
- Analgesic Efficacy of The Cyclooxygenase-2Specific Inhibitor Rofecoxib in Post-Dental Surgery Pain: A Randomized, Controlled TrialDocument11 pagesAnalgesic Efficacy of The Cyclooxygenase-2Specific Inhibitor Rofecoxib in Post-Dental Surgery Pain: A Randomized, Controlled TrialLeo AlbertoPas encore d'évaluation
- EpinephrineDocument5 pagesEpinephrinesheynnaPas encore d'évaluation
- Eledjam1991 Article BrachialPlexusBlockWithBupivac PDFDocument6 pagesEledjam1991 Article BrachialPlexusBlockWithBupivac PDFKalpanaPas encore d'évaluation
- RCT Parecoxib Acetaminophen...Document7 pagesRCT Parecoxib Acetaminophen...Paulina MuñozPas encore d'évaluation
- The Effects of Anesthetic Technique On Postoperative Opioid Consumption in Ankle Fracture SurgeryDocument16 pagesThe Effects of Anesthetic Technique On Postoperative Opioid Consumption in Ankle Fracture SurgeryGio VandaPas encore d'évaluation
- International Journal of Anesthetics and Anesthesiology Ijaa 7 118Document7 pagesInternational Journal of Anesthetics and Anesthesiology Ijaa 7 118Ferdy RahadiyanPas encore d'évaluation
- Efficacy of Dexamethasone For Reducing Postoperative Nausea and Vomiting and Analgesic Requirements After ThyroidectomyDocument4 pagesEfficacy of Dexamethasone For Reducing Postoperative Nausea and Vomiting and Analgesic Requirements After ThyroidectomyDr shehwarPas encore d'évaluation
- The Impact of Preemptive Perianal Anaesthetic Block in Open Haemorrhoidectomy - A Randomised Controlled TrialDocument3 pagesThe Impact of Preemptive Perianal Anaesthetic Block in Open Haemorrhoidectomy - A Randomised Controlled TrialhrtfdnbzvwPas encore d'évaluation
- Small-Dose Ketamine Infusion Improves Postoperative Analgesia and Rehabilitation After Total Knee ArthroplastyDocument6 pagesSmall-Dose Ketamine Infusion Improves Postoperative Analgesia and Rehabilitation After Total Knee ArthroplastyArturo AlcantaraPas encore d'évaluation
- Effect of Ketofol On Pain and Complication After Caesarean Delivery Under Spinal Anaesthesia: A Randomized Double-Blind Clinical TrialDocument4 pagesEffect of Ketofol On Pain and Complication After Caesarean Delivery Under Spinal Anaesthesia: A Randomized Double-Blind Clinical TrialHaryoko AnandaputraPas encore d'évaluation
- Asfr 2 QrqwasfcagsevDocument6 pagesAsfr 2 QrqwasfcagsevkennydimitraPas encore d'évaluation
- Efficacy Lidocaine Endoscopic Submucosal DissectionDocument7 pagesEfficacy Lidocaine Endoscopic Submucosal DissectionAnonymous lSWQIQPas encore d'évaluation
- Is Ginger Effective in Reducing Post-Tonsillectomy Morbidity? A Prospective Randomised Clinical TrialDocument6 pagesIs Ginger Effective in Reducing Post-Tonsillectomy Morbidity? A Prospective Randomised Clinical TrialRenaldyTandraPas encore d'évaluation
- Postoperative Nausea and Vomiting in OpioidFree Anesthesia Versus Opioid Based Anesthesia in Laparoscopic CholecystectomyDocument8 pagesPostoperative Nausea and Vomiting in OpioidFree Anesthesia Versus Opioid Based Anesthesia in Laparoscopic Cholecystectomypepe4dwinPas encore d'évaluation
- 10.1007@s00405 020 05801 6Document6 pages10.1007@s00405 020 05801 6Leonardo GuimelPas encore d'évaluation
- 2264-Article Text-5024-4-10-20151024Document6 pages2264-Article Text-5024-4-10-20151024shivamPas encore d'évaluation
- Acta Anaesthesiologica Taiwanica: Research PaperDocument6 pagesActa Anaesthesiologica Taiwanica: Research PaperStela MpPas encore d'évaluation
- Epiduroscopy Transforaminal Egyptian Society of Pain Ahmed El MollaDocument12 pagesEpiduroscopy Transforaminal Egyptian Society of Pain Ahmed El MollaProf. Dr. Ahmed El MollaPas encore d'évaluation
- Effect of Dexamethasone On The Duration of Interscalene Nerve Blocks With Ropivacaine or BupivacaineDocument8 pagesEffect of Dexamethasone On The Duration of Interscalene Nerve Blocks With Ropivacaine or BupivacaineIda KatarinaPas encore d'évaluation
- SMW 10163 PDFDocument9 pagesSMW 10163 PDFAngela PagliusoPas encore d'évaluation
- Haloperidol Combined With DexamethasoneDocument6 pagesHaloperidol Combined With Dexamethasoneapi-741687858Pas encore d'évaluation
- Efficay TAP Block PDFDocument5 pagesEfficay TAP Block PDFMarius PapuricaPas encore d'évaluation
- Anasthesia 1Document7 pagesAnasthesia 1Rionald SitompulPas encore d'évaluation
- Results and Complications of Spinal Anesthesia in Percutaneous NephrolithotomyDocument4 pagesResults and Complications of Spinal Anesthesia in Percutaneous NephrolithotomyDella Puspita SariPas encore d'évaluation
- 617 08 16 ArticleDocument8 pages617 08 16 Articlewilliam lozaPas encore d'évaluation
- Early Postoperative ComplicationsDocument6 pagesEarly Postoperative Complications49hr84j7spPas encore d'évaluation
- Oral Rehydration Therapy For Preoperative Fluid and Electrolyte Man-AgementDocument9 pagesOral Rehydration Therapy For Preoperative Fluid and Electrolyte Man-AgementSasmira JamalPas encore d'évaluation
- Research ArticleDocument7 pagesResearch Articlenaljnaby9Pas encore d'évaluation
- p6 High Risk PatientDocument6 pagesp6 High Risk Patientika lindaPas encore d'évaluation
- Initial Experience Using Incisional Anesthetic Catheter in Abdominal Wall Ambulatory SurgeryDocument6 pagesInitial Experience Using Incisional Anesthetic Catheter in Abdominal Wall Ambulatory SurgeryilhamPas encore d'évaluation
- JAnaesthClinPharmacol312191-1284204 033402Document5 pagesJAnaesthClinPharmacol312191-1284204 033402Rusman Hadi RachmanPas encore d'évaluation
- The Addition of Clonidine To Bupivacaine in Combined Femoral-Sciatic Nerve Block For Anterior Cruciate Ligament ReconstructionDocument0 pageThe Addition of Clonidine To Bupivacaine in Combined Femoral-Sciatic Nerve Block For Anterior Cruciate Ligament Reconstructionpshz92Pas encore d'évaluation
- Amalia 163216 - Journal ReadingDocument26 pagesAmalia 163216 - Journal ReadingGhifari FarandiPas encore d'évaluation
- TNF TreatmentDocument9 pagesTNF Treatmentachal12Pas encore d'évaluation
- Dr. - Nataraj - EJCM 132 1888 1893 2023Document7 pagesDr. - Nataraj - EJCM 132 1888 1893 2023vithz kPas encore d'évaluation
- Jurnal 2Document9 pagesJurnal 2Muhammad AgussalimPas encore d'évaluation
- Medi 96 E8514Document4 pagesMedi 96 E8514Syd BarretPas encore d'évaluation
- Effectiveness of Epidural Blood Patch in The Management of Post-Dural Puncture HeadacheDocument6 pagesEffectiveness of Epidural Blood Patch in The Management of Post-Dural Puncture HeadacheFabiola Valdez MaldonadoPas encore d'évaluation
- Piis0007091217365649Document6 pagesPiis0007091217365649I Made AryanaPas encore d'évaluation
- Aep 338Document9 pagesAep 338Luifer AgudeloPas encore d'évaluation
- Batoz 2009 Acute-PainDocument2 pagesBatoz 2009 Acute-PainOmar BazalduaPas encore d'évaluation
- Research ArticleDocument10 pagesResearch ArticlethiaPas encore d'évaluation
- Comparison of Preventive Analgesia Techniques in Circumcision Cases Dorsal Penile Nerve Block, Caudal Block, or Subcutaneous MorphineDocument7 pagesComparison of Preventive Analgesia Techniques in Circumcision Cases Dorsal Penile Nerve Block, Caudal Block, or Subcutaneous MorphinenatamkpPas encore d'évaluation
- Ameeta Joshi:, Eleni Parara, Tatiana V. MacfarlaneDocument8 pagesAmeeta Joshi:, Eleni Parara, Tatiana V. MacfarlaneGustavo RodríguezPas encore d'évaluation
- Jimbo 2017Document15 pagesJimbo 2017Sahily MoralesPas encore d'évaluation
- Br. J. Anaesth.-2009-Foss-111-6Document6 pagesBr. J. Anaesth.-2009-Foss-111-6alejandropst1664Pas encore d'évaluation
- Ağrısız Gastroskopi Sırasında Anestezi Indüksiyonunda Bireyselleştirilmiş Optimal Hedef Konsantrasyonu Hesaplamak Için Bir Gösterge Olarak Kirpik Refleksini Kullanmanın Uygulanabilirliğini Araştırmak.Document4 pagesAğrısız Gastroskopi Sırasında Anestezi Indüksiyonunda Bireyselleştirilmiş Optimal Hedef Konsantrasyonu Hesaplamak Için Bir Gösterge Olarak Kirpik Refleksini Kullanmanın Uygulanabilirliğini Araştırmak.Ali ÖzdemirPas encore d'évaluation
- Abuelyazed 2016Document7 pagesAbuelyazed 2016AYŞE GÜLŞAH ATASEVERPas encore d'évaluation
- Intravenous Ketorolac Vs Diclofenac For AnalgesiaDocument6 pagesIntravenous Ketorolac Vs Diclofenac For AnalgesiaMuhammad AgussalimPas encore d'évaluation
- JAnaesthClinPharmacol294459-335648 091924 PDFDocument6 pagesJAnaesthClinPharmacol294459-335648 091924 PDFaltaikhsannurPas encore d'évaluation
- Comparative Study of Epidural Fentanyl and Buprenorphine For Post Operative Analgesia in Lower Abdominal and Lower Limb SurgeriesDocument8 pagesComparative Study of Epidural Fentanyl and Buprenorphine For Post Operative Analgesia in Lower Abdominal and Lower Limb SurgeriesIOSRjournalPas encore d'évaluation
- Practice Advisory On The Appropriate Use of Nsaids in Primary CareDocument15 pagesPractice Advisory On The Appropriate Use of Nsaids in Primary CareAsti IndriyaniPas encore d'évaluation
- Nonsteroidal Anti-Inflammatory Drugs, Disease-Modifying Antirheumatic Drugs, Nonopiod Analgesics, & Drugs Used in GoutDocument1 pageNonsteroidal Anti-Inflammatory Drugs, Disease-Modifying Antirheumatic Drugs, Nonopiod Analgesics, & Drugs Used in GoutLuna Abigail TorresPas encore d'évaluation
- Nama ObatDocument12 pagesNama Obatrolin novitaPas encore d'évaluation
- Unitatea de Măsură Cantitate A Preț Unitar, LeiDocument14 pagesUnitatea de Măsură Cantitate A Preț Unitar, LeivictorPas encore d'évaluation
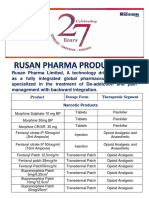
- Rusan Pharma Product ListDocument4 pagesRusan Pharma Product ListSanjay SharmaPas encore d'évaluation
- Lasa ListDocument11 pagesLasa ListerpPas encore d'évaluation
- Laporan Rak NarkotikaDocument18 pagesLaporan Rak NarkotikaaliyahPas encore d'évaluation
- Laporan Fornas Non FornasDocument6 pagesLaporan Fornas Non FornasrestyPas encore d'évaluation
- Opioids: Zainab Sabrie Pharmd MpharmDocument32 pagesOpioids: Zainab Sabrie Pharmd MpharmCabdiladif Ahmed McrfPas encore d'évaluation
- 13-Opioids Lecture 1Document41 pages13-Opioids Lecture 1api-343631539100% (1)
- AnalgesicDocument62 pagesAnalgesicAnjum IslamPas encore d'évaluation
- Opioid Analgesics and AntagonistsDocument8 pagesOpioid Analgesics and AntagonistsNishant KatiyarPas encore d'évaluation
- Miller's Drug Delivery SystemsDocument1 pageMiller's Drug Delivery SystemsNandor KissPas encore d'évaluation
- Ketamin Dan Blok Peritonsiler Untuk Penatalaksanaan Nyeri Post OperasiDocument6 pagesKetamin Dan Blok Peritonsiler Untuk Penatalaksanaan Nyeri Post OperasiranirahmaniPas encore d'évaluation
- Jeffrey L. Leal, MDDocument36 pagesJeffrey L. Leal, MDmemelandPas encore d'évaluation
- Anesthesia Hold List-MedicineDocument2 pagesAnesthesia Hold List-MedicineYogeswary RamachandranPas encore d'évaluation
- Codigos de Productos para SabanaDocument12 pagesCodigos de Productos para Sabanamarlenypilar30Pas encore d'évaluation
- Controlled Substances in Alphabetical OrderDocument17 pagesControlled Substances in Alphabetical Orderthor888888Pas encore d'évaluation
- DUROGESICDocument17 pagesDUROGESICshandybtPas encore d'évaluation
- Daftar Obat PrekusorDocument4 pagesDaftar Obat PrekusornovamunikaPas encore d'évaluation
- WHO Step Ladder For PainDocument5 pagesWHO Step Ladder For PainRizKyImanSariPas encore d'évaluation
- INCB Yellow ListDocument23 pagesINCB Yellow Listsunil_vaman_joshiPas encore d'évaluation
- Ace InhibitorsDocument15 pagesAce InhibitorsCarolyn Conn EdwardsPas encore d'évaluation
- I II III IV V: Description Examples ScheduleDocument1 pageI II III IV V: Description Examples ScheduleAndre PrayogoPas encore d'évaluation
- 9.4.48. 2004 Farre Paracetamol DOLORDocument12 pages9.4.48. 2004 Farre Paracetamol DOLORMonserrat Bello VargasPas encore d'évaluation
- OpioidsDocument29 pagesOpioidsHassan Jahangir100% (1)
- Anti Inflammatory DrugsDocument90 pagesAnti Inflammatory Drugsdrnasim2008817160% (5)
- SO Jan SepDocument28 pagesSO Jan SepApotek FazaPas encore d'évaluation
- Step Ladder in Pain Management (Dr. YNS)Document39 pagesStep Ladder in Pain Management (Dr. YNS)Erick Rangga JuniorPas encore d'évaluation
- Medicine ListDocument14 pagesMedicine Listapi-319888855Pas encore d'évaluation