Vous aimerez peut-être aussi
- Pathogens - TRAINING IN MICROBIOLOGICAL ANALYSIS OF FOODDocument52 pagesPathogens - TRAINING IN MICROBIOLOGICAL ANALYSIS OF FOODclairealbertiniPas encore d'évaluation
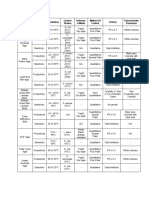
- Media Function Incubation Control Strains Referenc e Media Method of Control Criteria Characteristic ReactionsDocument2 pagesMedia Function Incubation Control Strains Referenc e Media Method of Control Criteria Characteristic ReactionsclairealbertiniPas encore d'évaluation
- Flowchart - Media QCDocument1 pageFlowchart - Media QCclairealbertiniPas encore d'évaluation
- HACCP Decision Tree PDFDocument1 pageHACCP Decision Tree PDFclairealbertiniPas encore d'évaluation
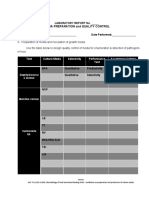
- Media Preparation and Quality ControlDocument3 pagesMedia Preparation and Quality ControlclairealbertiniPas encore d'évaluation
- Building-Up Competency On Color Analysis Using Visual Evaluation - Article For FNRI 2017 Annual Report - ColorDocument3 pagesBuilding-Up Competency On Color Analysis Using Visual Evaluation - Article For FNRI 2017 Annual Report - ColorclairealbertiniPas encore d'évaluation
- Module 1 - Water - TRAINING IN MICROBIOLOGY PDFDocument40 pagesModule 1 - Water - TRAINING IN MICROBIOLOGY PDFclairealbertiniPas encore d'évaluation
- SOP-4.3-2-0 Creation, Revision and Approval of DocumentsDocument4 pagesSOP-4.3-2-0 Creation, Revision and Approval of DocumentsclairealbertiniPas encore d'évaluation
- Ethical and Professional Practices For The Sensory Analysis of FoodsDocument3 pagesEthical and Professional Practices For The Sensory Analysis of Foodsclairealbertini100% (1)
- SOP-5.10 - Conduct of Sensory Evaluation (With IQC)Document8 pagesSOP-5.10 - Conduct of Sensory Evaluation (With IQC)clairealbertini100% (5)
- SOP 4.3 1 0 Control of DocumentsDocument4 pagesSOP 4.3 1 0 Control of DocumentsclairealbertiniPas encore d'évaluation
- Same-Different Test Analysis Using Chi-SquareDocument4 pagesSame-Different Test Analysis Using Chi-SquareclairealbertiniPas encore d'évaluation
- Monthly Performance Output Report Form 2Document1 pageMonthly Performance Output Report Form 2clairealbertiniPas encore d'évaluation
- Enhanced Sensory Evaluation Laboratory SoftwareDocument2 pagesEnhanced Sensory Evaluation Laboratory SoftwareclairealbertiniPas encore d'évaluation
- SOP-5.2-2-0 Recruitmen, Screening and Selection of Candidate Sensory PanelistsDocument2 pagesSOP-5.2-2-0 Recruitmen, Screening and Selection of Candidate Sensory Panelistsclairealbertini67% (3)
- Standard Operating Procedures On Assessment of Staff Training and CompetencyDocument4 pagesStandard Operating Procedures On Assessment of Staff Training and Competencyclairealbertini50% (6)
- Steps in Sensory EvaluationDocument1 pageSteps in Sensory Evaluationclairealbertini100% (1)
- Sensory Science 101 by IFT - How Do We TasteDocument13 pagesSensory Science 101 by IFT - How Do We TasteclairealbertiniPas encore d'évaluation
- Procedure For Isolation of Listeria MonocytogenesDocument5 pagesProcedure For Isolation of Listeria MonocytogenesclairealbertiniPas encore d'évaluation
- Sensory Science 101 by IFT - How Do We SmellDocument11 pagesSensory Science 101 by IFT - How Do We SmellclairealbertiniPas encore d'évaluation
- Personnel Training Plan and Record On Equipment OperationDocument1 pagePersonnel Training Plan and Record On Equipment Operationclairealbertini100% (1)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Tssttvdaf1 BDocument22 pagesTssttvdaf1 BAlejandro DiazPas encore d'évaluation
- Pre Ut U11sDocument2 pagesPre Ut U11sSvetlanaPas encore d'évaluation
- New Premium Veg Menu The Grand GourmetDocument6 pagesNew Premium Veg Menu The Grand GourmetPankaj MishraPas encore d'évaluation
- FSSAI Regulations On Food ColoursDocument2 pagesFSSAI Regulations On Food ColoursMadhu ShaliniPas encore d'évaluation
- Wahlburgers MenuDocument2 pagesWahlburgers MenuJose JaramilloPas encore d'évaluation
- What Are Herbs and Spices?: Plant Products That Are Added To Food or Drink To Provide AvorDocument24 pagesWhat Are Herbs and Spices?: Plant Products That Are Added To Food or Drink To Provide AvorAshish MakPas encore d'évaluation
- Aam Ka Kuchla 2 WaysDocument8 pagesAam Ka Kuchla 2 WaysAnonymous XuFb6TPas encore d'évaluation
- Industriya NG AsukalDocument12 pagesIndustriya NG AsukalJhamela Ann ElesterioPas encore d'évaluation
- Ava Is VeganDocument7 pagesAva Is Vegantutorial 001Pas encore d'évaluation
- Free WAEC Catering Craft Practice Past QuestionsDocument7 pagesFree WAEC Catering Craft Practice Past QuestionsCharles Obaleagbon0% (1)
- Project Plan For Soup and SauceDocument3 pagesProject Plan For Soup and SauceRenee Pintor0% (1)
- Consumer Reports Arsenic in Food November 2012 - 1Document1 pageConsumer Reports Arsenic in Food November 2012 - 1Maxvico100% (1)
- Week 5 Module Bread and PastryDocument7 pagesWeek 5 Module Bread and PastryJoan Dela CruzPas encore d'évaluation
- r2 Que-Barb Food-Menu 8.5x14 No PricesDocument1 pager2 Que-Barb Food-Menu 8.5x14 No PricesFarley ElliottPas encore d'évaluation
- Rearrange Jumbled WordsDocument2 pagesRearrange Jumbled WordsAdit AmbadiPas encore d'évaluation
- ROQUETTE-Quality-Product Information-Intolerance Agents Allergens-Maltodextrin-ENDocument2 pagesROQUETTE-Quality-Product Information-Intolerance Agents Allergens-Maltodextrin-ENakash kumarPas encore d'évaluation
- Team 8Document22 pagesTeam 8LaVette LaGonPas encore d'évaluation
- Lantana BreakfastDocument2 pagesLantana BreakfastMax MaximPas encore d'évaluation
- Prepare Vegetable, Fruit, Eggs and Farinaceous Dishes SITHCCC008 - PowerpointDocument78 pagesPrepare Vegetable, Fruit, Eggs and Farinaceous Dishes SITHCCC008 - PowerpointJuan Diego Pulgarín Henao75% (4)
- Lehmans Catalog Spring 2018Document72 pagesLehmans Catalog Spring 2018lowtech4100% (1)
- Blue Jasmine Event Package 2021Document20 pagesBlue Jasmine Event Package 2021wahyu nugrohoPas encore d'évaluation
- ProductsDocument2 pagesProductsCieloPas encore d'évaluation
- Philippine Coconut and Oil Palm Commodity Prices: Monthly Average For FEBRUARY 2019Document1 pagePhilippine Coconut and Oil Palm Commodity Prices: Monthly Average For FEBRUARY 2019Donnalyn VillamorPas encore d'évaluation
- Grilling Times Temperatures PDFDocument2 pagesGrilling Times Temperatures PDFMule148Pas encore d'évaluation
- Black Butte PorterDocument3 pagesBlack Butte Porterwihangnam78996Pas encore d'évaluation
- Beers: Finals-HMELEC 3Document6 pagesBeers: Finals-HMELEC 3CausePas encore d'évaluation
- Survival Creole: Bryant C. Freeman, PH.DDocument36 pagesSurvival Creole: Bryant C. Freeman, PH.DjaPas encore d'évaluation
- Chocolate Cake With Chocolate Mousse Filling - Tastes Better From ScratchDocument2 pagesChocolate Cake With Chocolate Mousse Filling - Tastes Better From ScratchGloria De la CruzPas encore d'évaluation
- Kabsa Recipe - Chicken Kabsa - Arab Rice RecipeDocument5 pagesKabsa Recipe - Chicken Kabsa - Arab Rice Recipesuresh0% (1)
- Class 7 Homework ReadingDocument1 pageClass 7 Homework ReadingFranco Aponte García100% (1)