Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- How To Play Blues UkeleleDocument0 pageHow To Play Blues Ukelelevidaldoval100% (4)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Excellent Research Paper On Boko HaramDocument38 pagesExcellent Research Paper On Boko HaramChad WhiteheadPas encore d'évaluation
- Yes Women FantasizeDocument6 pagesYes Women Fantasizevirad25Pas encore d'évaluation
- (Bereczkei, Tams) The SZONDI's LEGACY Innate Dispositions Influence Our ChoicesDocument17 pages(Bereczkei, Tams) The SZONDI's LEGACY Innate Dispositions Influence Our ChoicesVitor Gonçalves BarbosaPas encore d'évaluation
- OKC Bombing RevelationsDocument135 pagesOKC Bombing RevelationsChad Whitehead100% (1)
- Decibel - Direct Game cd2 Id1677117548 Size1967 PDFDocument182 pagesDecibel - Direct Game cd2 Id1677117548 Size1967 PDFDutch Van der LindePas encore d'évaluation
- Sample Petition - Recognition of Foreign Divorce DecreeDocument6 pagesSample Petition - Recognition of Foreign Divorce DecreeDeurod Inovejas100% (1)
- Black Lives Matter GoalsDocument2 pagesBlack Lives Matter GoalsChad Whitehead0% (1)
- Joint Chiefs of Staff Document RecomendationsDocument14 pagesJoint Chiefs of Staff Document RecomendationsChad WhiteheadPas encore d'évaluation
- Quizon Vs SaludDocument6 pagesQuizon Vs SaludJoseph PamaongPas encore d'évaluation
- Factors That Influence Postpartum RecoveryDocument2 pagesFactors That Influence Postpartum RecoveryHelenice Assis VespasianoPas encore d'évaluation
- The Development of The English LanguageDocument40 pagesThe Development of The English Languagetrythispie100% (2)
- Fourteen Scholarship Essay Examples That Won Thousands 2018-1Document16 pagesFourteen Scholarship Essay Examples That Won Thousands 2018-114Nyayu Aisha Almira ApriliaPas encore d'évaluation
- The Slight Incline of The Big Pig Porkers. Anthony JonesDocument7 pagesThe Slight Incline of The Big Pig Porkers. Anthony Jonesapi-150837007100% (1)
- Boko Haram Teaching ResourceDocument10 pagesBoko Haram Teaching ResourceChad WhiteheadPas encore d'évaluation
- HRW Boko HaramDocument69 pagesHRW Boko HaramChad WhiteheadPas encore d'évaluation
- Thomson Boko HaramDocument15 pagesThomson Boko HaramChad WhiteheadPas encore d'évaluation
- 2012 1009 RomneyAgricultureDocument16 pages2012 1009 RomneyAgricultureChad WhiteheadPas encore d'évaluation
- Conventions Summaries Private International LawDocument16 pagesConventions Summaries Private International LawpinoydooyeweerdianPas encore d'évaluation
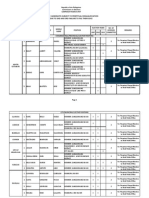
- Candidate Who File Their SOCE Two or More Elections R12Document9 pagesCandidate Who File Their SOCE Two or More Elections R12Norai TalbinPas encore d'évaluation
- Who Are Social WorkersDocument6 pagesWho Are Social WorkersDavidPongoPas encore d'évaluation
- 101 ReadingDocument26 pages101 ReadingNedal Abi OrmPas encore d'évaluation
- Isidro Ablaza Vs - Republic of The PhilippinesDocument1 pageIsidro Ablaza Vs - Republic of The PhilippinesPaco RomanPas encore d'évaluation
- P L Sayal V Sarla Rani Case PresentationDocument2 pagesP L Sayal V Sarla Rani Case PresentationJhasha KorraPas encore d'évaluation
- William Wordsworth and The DaffodilsDocument2 pagesWilliam Wordsworth and The Daffodilscucdtk87Pas encore d'évaluation
- Changing Nature of Interpersonal Relationships in A Female PrisonDocument27 pagesChanging Nature of Interpersonal Relationships in A Female PrisonStephen PopePas encore d'évaluation
- The Use of Search Engines Learning Competency: Use Search Engines To Conduct A Guided Search On A Given Topic. EN7SS-II-c-1.5.3Document7 pagesThe Use of Search Engines Learning Competency: Use Search Engines To Conduct A Guided Search On A Given Topic. EN7SS-II-c-1.5.3Muzfa Palattao MangasilPas encore d'évaluation
- Ficha 01 - Und 05 - Semana 1 - Clase 1 - Jer Rur - 5° - Miss AydaDocument2 pagesFicha 01 - Und 05 - Semana 1 - Clase 1 - Jer Rur - 5° - Miss AydaRocio Del Pilar MariñasPas encore d'évaluation
- A2 Film Studies Essay FinalDocument7 pagesA2 Film Studies Essay FinaltahjahPas encore d'évaluation
- New York's Little Italy, Littler by The Year #88Document4 pagesNew York's Little Italy, Littler by The Year #88imsungbaekPas encore d'évaluation
- A Critical Analysis of The Right of CoparcenerDocument27 pagesA Critical Analysis of The Right of CoparcenerSHUBHAM RAJPas encore d'évaluation
- Spec Pro Page 2 of 6Document39 pagesSpec Pro Page 2 of 6mccm92Pas encore d'évaluation
- Final Test - Attempt ReviewDocument4 pagesFinal Test - Attempt Reviewnatasha murilloPas encore d'évaluation
- Classic Films You Must See: The GodfatherDocument1 pageClassic Films You Must See: The GodfatherOdett OszlánszkiPas encore d'évaluation
- Flower MorphologyDocument129 pagesFlower MorphologySleeping Beauty100% (1)
- Deviance EssayDocument2 pagesDeviance EssayAbbiegail Nicole AbinalPas encore d'évaluation
- Indo-European Words Nipple, Nimbu and NimbaDocument11 pagesIndo-European Words Nipple, Nimbu and NimbaPremendra Priyadarshi100% (1)
- G.R. No. 214529 JERRYSUS L. TILAR, Petitioner Elizabeth A. Tilar and The Republic of The Philippines, Respondents Decision Peralta, J.Document4 pagesG.R. No. 214529 JERRYSUS L. TILAR, Petitioner Elizabeth A. Tilar and The Republic of The Philippines, Respondents Decision Peralta, J.jbandPas encore d'évaluation