Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Barbaric Rites v1Document14 pagesBarbaric Rites v1dm66689% (9)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Student Exploration: Identifying NutrientsDocument4 pagesStudent Exploration: Identifying NutrientsDarcy DunganPas encore d'évaluation
- Ijeb 48 (7) 642-650Document9 pagesIjeb 48 (7) 642-650dedypurnamaPas encore d'évaluation
- Intoxication GuidelinesDocument3 pagesIntoxication GuidelinesdedypurnamaPas encore d'évaluation
- 51 Tips For Excessive Sweating PDFDocument10 pages51 Tips For Excessive Sweating PDFdedypurnamaPas encore d'évaluation
- Special TopicDocument7 pagesSpecial TopicdedypurnamaPas encore d'évaluation
- (Melastoma Malabathricum L.), Moist Exposed Burn Ointment (MEBO) andDocument2 pages(Melastoma Malabathricum L.), Moist Exposed Burn Ointment (MEBO) anddedypurnamaPas encore d'évaluation
- A Toolkit For Women's Empowerment and Leadership in Health and WelfareDocument56 pagesA Toolkit For Women's Empowerment and Leadership in Health and WelfarededypurnamaPas encore d'évaluation
- Corneal Transplantation at An Ophthalmological Referral Center in Colombia: Indications and Techniques (2004-2011)Document4 pagesCorneal Transplantation at An Ophthalmological Referral Center in Colombia: Indications and Techniques (2004-2011)dedypurnamaPas encore d'évaluation
- A Case of Choroidal Neovascularization Secondary To Unilateral Retinal Pigment Epithelium DysgenesisDocument4 pagesA Case of Choroidal Neovascularization Secondary To Unilateral Retinal Pigment Epithelium DysgenesisdedypurnamaPas encore d'évaluation
- Refractive Surgery: The Never Ending Task of Improving Vision CorrectionDocument2 pagesRefractive Surgery: The Never Ending Task of Improving Vision CorrectiondedypurnamaPas encore d'évaluation
- 83 Healthy Recipe SubstitutionsDocument14 pages83 Healthy Recipe SubstitutionsManuela Lidia Pitis MorosanuPas encore d'évaluation
- 2010 05 25 0848472010 - CaluscusinDocument50 pages2010 05 25 0848472010 - CaluscusinAchmad Deddy FatoniPas encore d'évaluation
- Bu LesDocument91 pagesBu LesAnonymous zQ72D9cPrCPas encore d'évaluation
- Ejer HipotesisDocument17 pagesEjer HipotesissoryPas encore d'évaluation
- Hcin 541 Final Project Term PaperDocument12 pagesHcin 541 Final Project Term Paperapi-464801402Pas encore d'évaluation
- Session 4Document7 pagesSession 4SandyPas encore d'évaluation
- 2017 Hypertension Webinar PDFDocument81 pages2017 Hypertension Webinar PDFMira Mariana UlfahPas encore d'évaluation
- What Every Baker Needs To Know About SugarDocument14 pagesWhat Every Baker Needs To Know About SugarBe ChahPas encore d'évaluation
- Insanity Workout Excel WorksheetDocument3 pagesInsanity Workout Excel WorksheetBrian BishopPas encore d'évaluation
- Required: Body System: Session Topic: Educational Format Faculty Expertise RequiredDocument16 pagesRequired: Body System: Session Topic: Educational Format Faculty Expertise RequiredThaysa LimaPas encore d'évaluation
- Facts and Definition of EclampsiaDocument5 pagesFacts and Definition of EclampsiaChoi Gong JuPas encore d'évaluation
- Front Lever Tutorial 4ab8cfea A19b 4f83 A596 A22faf632941Document23 pagesFront Lever Tutorial 4ab8cfea A19b 4f83 A596 A22faf632941jasoo__100% (6)
- APPETITE: Physiological and Neurobiological AspectsDocument8 pagesAPPETITE: Physiological and Neurobiological AspectsTamara Souza RossiPas encore d'évaluation
- Fitness Progress Chart For Men (Metric) 1Document4 pagesFitness Progress Chart For Men (Metric) 1John Gaming444Pas encore d'évaluation
- Eddy Wirawan, SPJP - Fiha: Rsud. Ulin BanjarmasinDocument49 pagesEddy Wirawan, SPJP - Fiha: Rsud. Ulin Banjarmasineka febriantyPas encore d'évaluation
- Jurnal Bahasa Inggris PDFDocument10 pagesJurnal Bahasa Inggris PDFRi Yudo ShotaroPas encore d'évaluation
- Guidelines For ArticleDocument3 pagesGuidelines For ArticlebokbokreonalPas encore d'évaluation
- ALPCO Announces Deadline For Winter 2020 Diabetes Research Travel Grant AwardDocument2 pagesALPCO Announces Deadline For Winter 2020 Diabetes Research Travel Grant AwardPR.comPas encore d'évaluation
- Regulation of Cholesterol SynthesisDocument20 pagesRegulation of Cholesterol SynthesisHusnaPas encore d'évaluation
- Nutritional Status StartDocument3 pagesNutritional Status StartJasully Tambong UlleguePas encore d'évaluation
- Public SpeakingDocument2 pagesPublic SpeakingKhai Onie100% (1)
- Androgenetic Alopecia and Coronary Artery Disease CASE CONTROL STUDY DR RAHUL KUMAR SHARMA SKIN SPECIALIST AJMERDocument2 pagesAndrogenetic Alopecia and Coronary Artery Disease CASE CONTROL STUDY DR RAHUL KUMAR SHARMA SKIN SPECIALIST AJMERRahul SharmaPas encore d'évaluation
- Get Up & Grow Healthy Eating and Physical Activity For Early ChildhoodDocument3 pagesGet Up & Grow Healthy Eating and Physical Activity For Early ChildhoodAarón LinaresPas encore d'évaluation
- NeuropatiDocument36 pagesNeuropatirenato raziPas encore d'évaluation
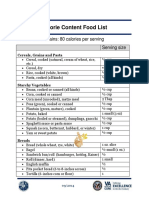
- Calorie Content Food ListDocument7 pagesCalorie Content Food ListOla Gf Olamit100% (1)
- Green SmoothieDocument20 pagesGreen Smoothieibrahim kamalPas encore d'évaluation
- Nutritional Applications in Exercise and Sport PDFDocument309 pagesNutritional Applications in Exercise and Sport PDFalexcesePas encore d'évaluation
- Sugar ExptDocument9 pagesSugar ExptShiva BhaskarPas encore d'évaluation