Vous aimerez peut-être aussi
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- Depression in The ElderlyDocument9 pagesDepression in The Elderlyscabrera_scribd100% (1)
- WFSBP Consensus Paper Biological Markers in DepressionDocument34 pagesWFSBP Consensus Paper Biological Markers in Depressionscabrera_scribdPas encore d'évaluation
- 2014 SAra Piras - Prediction and Prevention of The First Psychotic, New DirectionDocument13 pages2014 SAra Piras - Prediction and Prevention of The First Psychotic, New Directionscabrera_scribdPas encore d'évaluation
- WFBSP SZ Guidelines Part2 2013 Long Tgerm SchiDocument43 pagesWFBSP SZ Guidelines Part2 2013 Long Tgerm Schiscabrera_scribdPas encore d'évaluation
- WFBSP SZ Guidelines Part1 2012 Acute SchizophreniaDocument61 pagesWFBSP SZ Guidelines Part1 2012 Acute Schizophreniascabrera_scribdPas encore d'évaluation
- Psychopathology Consensus StatementDocument8 pagesPsychopathology Consensus Statementscabrera_scribdPas encore d'évaluation
- Guidelines Anxiety RevisionDocument65 pagesGuidelines Anxiety Revisionscabrera_scribdPas encore d'évaluation
- Depression 2Document18 pagesDepression 2scabrera_scribdPas encore d'évaluation
- Aigner WFSBP Guidelines Eating Disorder World J Biol Psychia 11Document44 pagesAigner WFSBP Guidelines Eating Disorder World J Biol Psychia 11scabrera_scribdPas encore d'évaluation
- The World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines For The Biological Treatment of Bipolar Disorders: Update 2009 On The Treatment of Acute ManiaDocument32 pagesThe World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines For The Biological Treatment of Bipolar Disorders: Update 2009 On The Treatment of Acute Maniascabrera_scribdPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- LECTURE NOTES For Health Science StudentDocument211 pagesLECTURE NOTES For Health Science StudentMohsinPas encore d'évaluation
- A Review of Antidiabetic Potential of Ethnomedicinal Plants 2167 0412.1000165Document8 pagesA Review of Antidiabetic Potential of Ethnomedicinal Plants 2167 0412.1000165Davia FendiePas encore d'évaluation
- The Essentials of Pain ManagementDocument46 pagesThe Essentials of Pain ManagementTaufik Akbar Faried LubisPas encore d'évaluation
- Annual Report 2018Document276 pagesAnnual Report 2018Unsinkable CatPas encore d'évaluation
- FILE STOK - OdsDocument162 pagesFILE STOK - OdsAhmad GupongPas encore d'évaluation
- Common Drugs in SA MedicineDocument8 pagesCommon Drugs in SA MedicineJordan PetersPas encore d'évaluation
- 3 Good Inventions SIMPLE PAST Aff To NegDocument1 page3 Good Inventions SIMPLE PAST Aff To NegvbpbPas encore d'évaluation
- Price List From 14.10.2013Document27 pagesPrice List From 14.10.2013jasoneinsteinPas encore d'évaluation
- Pharmacology Lab ManualDocument41 pagesPharmacology Lab ManualShardendu Mishra0% (1)
- Cyclobenzaprine Hydro ChlorideDocument2 pagesCyclobenzaprine Hydro Chlorideapi-3797941Pas encore d'évaluation
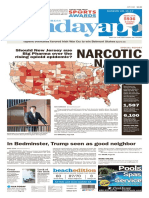
- Asbury Park Press Front Page, Sunday, June 11, 2017Document1 pageAsbury Park Press Front Page, Sunday, June 11, 2017Asbury Park PressPas encore d'évaluation
- CPW Drugs in PPMP Number of DuplictesDocument9 pagesCPW Drugs in PPMP Number of DuplictesSunshine BPas encore d'évaluation
- XareltofinalDocument2 pagesXareltofinalMuniba NasimPas encore d'évaluation
- Anti-Rheumatoid Arthritis DrugsDocument57 pagesAnti-Rheumatoid Arthritis Drugsapi-306036754Pas encore d'évaluation
- Featured Companies That Provide Contract ManufacturingDocument6 pagesFeatured Companies That Provide Contract Manufacturingvibhor_26janPas encore d'évaluation
- Himalaya HerbalsDocument45 pagesHimalaya HerbalsShraddha50% (2)
- Jam - 3 - 3 - 1 A Developed Process For The Synthesis of 2-Ethyl Phenyl Hydrazine Hydrochloride, A Key Starting Material For 7-Ethyl Tryptophol.Document4 pagesJam - 3 - 3 - 1 A Developed Process For The Synthesis of 2-Ethyl Phenyl Hydrazine Hydrochloride, A Key Starting Material For 7-Ethyl Tryptophol.jamonline100% (3)
- 04 Prescription InterpretationDocument32 pages04 Prescription InterpretationBalsam Zahi Al-HasanPas encore d'évaluation
- Researching Alzheimer's Medicines - Setbacks and Stepping StonesDocument20 pagesResearching Alzheimer's Medicines - Setbacks and Stepping StonesOscar EspinozaPas encore d'évaluation
- A Handbook of CosmeticsDocument134 pagesA Handbook of CosmeticsTo Ra100% (2)
- Target Niper ProspectusDocument31 pagesTarget Niper ProspectusJayesh DokePas encore d'évaluation
- Ramipril: SampleDocument4 pagesRamipril: SamplePapaindoPas encore d'évaluation
- Medical Waste Disposal Guidelines The Pharmacia de Medicina Will DisposeDocument4 pagesMedical Waste Disposal Guidelines The Pharmacia de Medicina Will DisposemfbaitecPas encore d'évaluation
- D Watson Chemists:: Pakistan German Business ForumDocument3 pagesD Watson Chemists:: Pakistan German Business ForumareebPas encore d'évaluation
- Sandoz 2010 - 2011 Pocket GuideDocument118 pagesSandoz 2010 - 2011 Pocket Guidemaheshgandla21Pas encore d'évaluation
- Journal Reading: Oleh: M. Isyhaduul Islam Arifiana Khusnul Hidayati Ulfi Shofahati Puskesmas GedongtengenDocument17 pagesJournal Reading: Oleh: M. Isyhaduul Islam Arifiana Khusnul Hidayati Ulfi Shofahati Puskesmas GedongtengenIka Wardhani KaruniaPas encore d'évaluation
- 2019 PHDDocument41 pages2019 PHDnarendar.1Pas encore d'évaluation
- Ijpab 2015 3 1 224 235 PDFDocument12 pagesIjpab 2015 3 1 224 235 PDFDrAmit VermaPas encore d'évaluation
- Dietary Supplements: What 'S in A Name? What's in The Bottle?Document3 pagesDietary Supplements: What 'S in A Name? What's in The Bottle?chrissPas encore d'évaluation
- Supply Chin Management of Himalaya CompanyDocument79 pagesSupply Chin Management of Himalaya Companysantunusoren80% (5)