Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Evolutionary Analysis of The Dynamics of Viral Infectious Disease.Document11 pagesEvolutionary Analysis of The Dynamics of Viral Infectious Disease.Sury Arias EscalantePas encore d'évaluation
- Clin Infect Dis. 2009 Staples 942 8Document7 pagesClin Infect Dis. 2009 Staples 942 8Sury Arias EscalantePas encore d'évaluation
- Mycoplasma GenitaliumDocument7 pagesMycoplasma GenitaliumSury Arias EscalantePas encore d'évaluation
- Effects of Caffeine in Parkinson Disease, 2010Document16 pagesEffects of Caffeine in Parkinson Disease, 2010Sury Arias EscalantePas encore d'évaluation
- Alineacion SHV1648Document11 pagesAlineacion SHV1648Sury Arias EscalantePas encore d'évaluation
- CDKS, Cyclins and CKIs Roles Beyond Cell Cycle Regulation. 2013Document15 pagesCDKS, Cyclins and CKIs Roles Beyond Cell Cycle Regulation. 2013Sury Arias EscalantePas encore d'évaluation
- Chikungunya in Las Americas PDFDocument3 pagesChikungunya in Las Americas PDFSury Arias EscalantePas encore d'évaluation
- Ng.08 Epigen RegDocument7 pagesNg.08 Epigen RegSury Arias EscalantePas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- EritropoesisDocument15 pagesEritropoesisFitriyani Dewi SuwandhiPas encore d'évaluation
- 3rd GRADING PERIODICAL EXAM MAPEH 8Document1 page3rd GRADING PERIODICAL EXAM MAPEH 8Amor BatasPas encore d'évaluation
- The Importance of Selenium To Human HealthDocument9 pagesThe Importance of Selenium To Human HealthIrma Melyani PuspitasariPas encore d'évaluation
- Resources 11 00015 v2Document20 pagesResources 11 00015 v2Gina M LópezPas encore d'évaluation
- Mechanisms of Drugs Action 2021 Full For MBBSDocument80 pagesMechanisms of Drugs Action 2021 Full For MBBSMARYAM ASIMPas encore d'évaluation
- Organic Feeds Using Indigenous Microbial Fermented Imf Feeds For Organic Free Range Native Pigs and ChickensDocument67 pagesOrganic Feeds Using Indigenous Microbial Fermented Imf Feeds For Organic Free Range Native Pigs and ChickenskarikambingPas encore d'évaluation
- Syllabus Gribble, BIOSC 0150, F14 PDFDocument5 pagesSyllabus Gribble, BIOSC 0150, F14 PDFasdjfkj4kljrjsPas encore d'évaluation
- Animalia Part 1 Invertebrata PDFDocument46 pagesAnimalia Part 1 Invertebrata PDFTiara Safa EarlenePas encore d'évaluation
- The association between acute asthma severity and peripheral blood inflammatory cellsDocument6 pagesThe association between acute asthma severity and peripheral blood inflammatory cellsFarel Muhammad Sayyaf HaydarPas encore d'évaluation
- Lesson 1 - Sex and GenderDocument5 pagesLesson 1 - Sex and Genderweyn feitPas encore d'évaluation
- Ecosystem: BY: Jamaica R. AsuncionDocument21 pagesEcosystem: BY: Jamaica R. AsuncionJamaica AsuncionPas encore d'évaluation
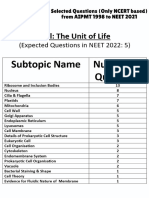
- Cell - The Unit of Life - NCERT Based PYQsDocument9 pagesCell - The Unit of Life - NCERT Based PYQsAkhil singhPas encore d'évaluation
- SR5 TOOL Chrome Flesh IndexDocument2 pagesSR5 TOOL Chrome Flesh IndexBeki LokaPas encore d'évaluation
- North Carolina Test of Biology: ReleasedDocument31 pagesNorth Carolina Test of Biology: ReleasedKamilla DzhanzakovaPas encore d'évaluation
- Grade 11 Topic TestsDocument100 pagesGrade 11 Topic TestsKïm MugarapajiwaPas encore d'évaluation
- Principles of Botany SyllabusDocument6 pagesPrinciples of Botany Syllabusjhdgkjdhfbb bbPas encore d'évaluation
- Bio Practicals 2022-23Document31 pagesBio Practicals 2022-23Aman AaryanPas encore d'évaluation
- HotLab Agustus 2019-DikonversiDocument71 pagesHotLab Agustus 2019-DikonversiEndy JuliantoPas encore d'évaluation
- PBL Haem 1Document9 pagesPBL Haem 1Mall Singh BhullarPas encore d'évaluation
- IGCSE Biology Revision Notes - Kingdoms, ClassificationDocument4 pagesIGCSE Biology Revision Notes - Kingdoms, ClassificationClara ToPas encore d'évaluation
- Biotechnology and Its ApplicationsDocument2 pagesBiotechnology and Its ApplicationsEunice BasarioPas encore d'évaluation
- No. Isbn VolDocument131 pagesNo. Isbn VolBayu SmadaPas encore d'évaluation
- W. James Kent - BLAT-The BLAST-Like Alignment ToolDocument10 pagesW. James Kent - BLAT-The BLAST-Like Alignment ToolYopghm698Pas encore d'évaluation
- Guinea Tropical Ecology and Biodiversity Digest Issue 13Document25 pagesGuinea Tropical Ecology and Biodiversity Digest Issue 13Leaks From BurmaPas encore d'évaluation
- Animal Kingdom Classification GuideDocument91 pagesAnimal Kingdom Classification GuideJoanna Susan JojiPas encore d'évaluation
- STS Module 8 Gene TheraphyDocument7 pagesSTS Module 8 Gene Theraphyjevieconsultaaquino2003Pas encore d'évaluation
- A Tool For The Analysis of Chromosomes: Karyotype: Taxon June 2016Document8 pagesA Tool For The Analysis of Chromosomes: Karyotype: Taxon June 2016Kelly Rios ZapataPas encore d'évaluation
- A Well Organized Human BodyDocument8 pagesA Well Organized Human BodyRain Klien BobisPas encore d'évaluation
- Government of Telangana Office of The Director of Public Health and Family WelfareDocument14 pagesGovernment of Telangana Office of The Director of Public Health and Family WelfareSidhu SidhPas encore d'évaluation
- Childhood MedulloblastmaDocument17 pagesChildhood MedulloblastmaIrenaPas encore d'évaluation