Vous aimerez peut-être aussi
- Telemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.D'EverandTelemedicine and Asthma: An innovative approach to improve morbidity and mortality rates for active adults.: Effects of Telemedicine in Asthma care for remote and inner-city underserved populations.Pas encore d'évaluation
- 2020-Indian Journal of Public Health Research and Development (Scopus Q-4)Document5 pages2020-Indian Journal of Public Health Research and Development (Scopus Q-4)NoniAndayaniPas encore d'évaluation
- Hypertension Prediction Using Machine Learning Algorithm Among Indonesian AdultsDocument9 pagesHypertension Prediction Using Machine Learning Algorithm Among Indonesian AdultsIAES IJAIPas encore d'évaluation
- Assessment of Knowledge of Osteoarthritis Among Elderly PatientsDocument7 pagesAssessment of Knowledge of Osteoarthritis Among Elderly PatientsMostafa ShabanPas encore d'évaluation
- A Data-Driven Approach To Predicting Diabetes and Cardiovascular Disease With Machine LearningDocument15 pagesA Data-Driven Approach To Predicting Diabetes and Cardiovascular Disease With Machine LearningKnowledgepoint KpPas encore d'évaluation
- Sample 2Document11 pagesSample 2Muhamad Fikri AzizPas encore d'évaluation
- AP Comparación PaisesDocument10 pagesAP Comparación PaisesMiguel Ángel Estévez PAzPas encore d'évaluation
- Diagnostics: A Machine-Learning-Based Prediction Method For Hypertension Outcomes Based On Medical DataDocument21 pagesDiagnostics: A Machine-Learning-Based Prediction Method For Hypertension Outcomes Based On Medical DatafarzanaPas encore d'évaluation
- Chronic Diseases and InjuriesDocument16 pagesChronic Diseases and InjuriesShama ChalkePas encore d'évaluation
- CVD Risk EstimationDocument8 pagesCVD Risk EstimationparthibanePas encore d'évaluation
- Prevalence of Stroke in The Elderly A Systematic Review and Meta-AnalysisDocument10 pagesPrevalence of Stroke in The Elderly A Systematic Review and Meta-AnalysisMarian J. NietoPas encore d'évaluation
- Post-Stroke Patients With Moderate Function Have The Greatest Risk of Falls: A National Cohort StudyDocument9 pagesPost-Stroke Patients With Moderate Function Have The Greatest Risk of Falls: A National Cohort Studyhari vijayPas encore d'évaluation
- ContentServer Psico1Document14 pagesContentServer Psico1Luis.fernando. GarciaPas encore d'évaluation
- Elsevier Article PaperDocument24 pagesElsevier Article Paperjaveriazia97Pas encore d'évaluation
- Proceedings ICHLSR Singapore, JuneDocument29 pagesProceedings ICHLSR Singapore, JuneGlobal Research and Development ServicesPas encore d'évaluation
- WHO CVD Risk FactorsDocument18 pagesWHO CVD Risk FactorsparthibanePas encore d'évaluation
- 2019 - Kang - Does A Mobile App Improve Patients'Document9 pages2019 - Kang - Does A Mobile App Improve Patients'Warsi MaryatiPas encore d'évaluation
- The Bioterrorism Preparedness and Response Early Aberration Reporting System (EARS)Document8 pagesThe Bioterrorism Preparedness and Response Early Aberration Reporting System (EARS)Jojo MarinayPas encore d'évaluation
- Medical Tribune January 2012 HKDocument72 pagesMedical Tribune January 2012 HKKarena SabadoPas encore d'évaluation
- Aids 33 s283Document12 pagesAids 33 s283ilhamfajriPas encore d'évaluation
- Life Expectancy Using Data AnalyticsDocument9 pagesLife Expectancy Using Data AnalyticsIJRASETPublications100% (1)
- TH 16024Document10 pagesTH 16024dnoksPas encore d'évaluation
- 2008 - Feigin - Long Term Neuropsychological Functional Outcomes StrokeDocument8 pages2008 - Feigin - Long Term Neuropsychological Functional Outcomes StrokeLourdes CFPas encore d'évaluation
- Effect of Lifestyle Modification Intervention On Health Status of Coronary Artery Disease Patients Randomized Control TrialDocument14 pagesEffect of Lifestyle Modification Intervention On Health Status of Coronary Artery Disease Patients Randomized Control TrialRobet Agung wicaksonoPas encore d'évaluation
- 14 - Towards Best Practice in Acute Stroke Care in Ghana A Survey of Hospital ServicesDocument11 pages14 - Towards Best Practice in Acute Stroke Care in Ghana A Survey of Hospital ServicesChristel CibalonzaPas encore d'évaluation
- A Hybrid Model For Forecasting Communicable Diseases in MaldivesDocument13 pagesA Hybrid Model For Forecasting Communicable Diseases in MaldivesMervat BamiahPas encore d'évaluation
- The Satisfactionof Patients On Maintenance Hemodialysis Concerning The Provided Nursing Care in Hemodialysis UnitsDocument11 pagesThe Satisfactionof Patients On Maintenance Hemodialysis Concerning The Provided Nursing Care in Hemodialysis Unitsbe a doctor for you Medical studentPas encore d'évaluation
- Stroke Risk Screening Scales (SRSS) : Identi Fication of Domain and Item GenerationDocument8 pagesStroke Risk Screening Scales (SRSS) : Identi Fication of Domain and Item Generationandi kurniawanPas encore d'évaluation
- J of Clinical Hypertension - 2019 - Kanegae - Highly Precise Risk Prediction Model For New Onset Hypertension UsingDocument6 pagesJ of Clinical Hypertension - 2019 - Kanegae - Highly Precise Risk Prediction Model For New Onset Hypertension UsingMarie VarangotPas encore d'évaluation
- Risk Factors, Clinical Presentations and Predictors of Stroke Among Adult Patients Admitted To Stroke Unit of Jimma University Medical Center, South West Ethiopia: Prospective Observational StudyDocument11 pagesRisk Factors, Clinical Presentations and Predictors of Stroke Among Adult Patients Admitted To Stroke Unit of Jimma University Medical Center, South West Ethiopia: Prospective Observational StudyReyhan AristoPas encore d'évaluation
- Prediction of Intracranial Aneurysm Risk Using Machine LearningDocument10 pagesPrediction of Intracranial Aneurysm Risk Using Machine LearningKiran KumarPas encore d'évaluation
- Assessment of Knowledge, Attitude and Practice of Health Information Management Professionals Towards Integrated Disease Surveillance & Response (IDSR) in Abuja, Nigeria.Document48 pagesAssessment of Knowledge, Attitude and Practice of Health Information Management Professionals Towards Integrated Disease Surveillance & Response (IDSR) in Abuja, Nigeria.Victor Chibueze IjeomaPas encore d'évaluation
- Knowledge, Practice, and Attitude Towards Deep Vein Thrombosis Prophylaxis Among Residents and Interns in King Saud Medical CityDocument8 pagesKnowledge, Practice, and Attitude Towards Deep Vein Thrombosis Prophylaxis Among Residents and Interns in King Saud Medical CityIJAR JOURNALPas encore d'évaluation
- Main 25Document6 pagesMain 25pokharelriwaj82Pas encore d'évaluation
- Assessment of Awareness of Diabetic Retinopathy Among Type 2 Diabetes Mellitus Cross Sectional Study From Central IndiaDocument7 pagesAssessment of Awareness of Diabetic Retinopathy Among Type 2 Diabetes Mellitus Cross Sectional Study From Central IndiaAthenaeum Scientific PublishersPas encore d'évaluation
- Out 9Document11 pagesOut 9restu anindityaPas encore d'évaluation
- Who 2016 PDFDocument2 pagesWho 2016 PDFRefialy WahyyPas encore d'évaluation
- 75-Article Text-329-1-10-20220929Document16 pages75-Article Text-329-1-10-20220929BrianPas encore d'évaluation
- The Burden of Antimicrobial Resistance (AMR) in IndonesiaDocument4 pagesThe Burden of Antimicrobial Resistance (AMR) in IndonesiaJeanny APas encore d'évaluation
- Healthcare 11 01803Document25 pagesHealthcare 11 01803Trang PhạmPas encore d'évaluation
- Press Release-COVID-19 Survey (1) 5-12-20Document5 pagesPress Release-COVID-19 Survey (1) 5-12-20Ravikiran SuryanarayanamurthyPas encore d'évaluation
- Evaluation of Stroke Rehabilitation Services in The In-Hospital Phase: Findings From A Tertiary Care Centre in IndiaDocument15 pagesEvaluation of Stroke Rehabilitation Services in The In-Hospital Phase: Findings From A Tertiary Care Centre in IndiaIJAR JOURNALPas encore d'évaluation
- Jurnal MuskuloDocument8 pagesJurnal MuskuloarvinelaPas encore d'évaluation
- 25FirouzAmani EtalDocument6 pages25FirouzAmani EtaleditorijmrhsPas encore d'évaluation
- BMC Public Health: Evaluation of Reporting Timeliness of Public Health Surveillance Systems For Infectious DiseasesDocument9 pagesBMC Public Health: Evaluation of Reporting Timeliness of Public Health Surveillance Systems For Infectious DiseasesAnis RanisPas encore d'évaluation
- Prevalence and Awareness of Hypertension in NigeriaDocument13 pagesPrevalence and Awareness of Hypertension in NigeriaTaoreed AdegokePas encore d'évaluation
- Impact of Big Data Analytics On People's Health: Overview of Systematic Reviews and Recommendations For Future StudiesDocument14 pagesImpact of Big Data Analytics On People's Health: Overview of Systematic Reviews and Recommendations For Future Studiesalemayehu badargaPas encore d'évaluation
- The Relationships Between Step Count and All-Cause Mortality and Cardiovascular Events A Dose-Response Meta-Analysis - 1-S2.0-S2095254621001010-MainDocument9 pagesThe Relationships Between Step Count and All-Cause Mortality and Cardiovascular Events A Dose-Response Meta-Analysis - 1-S2.0-S2095254621001010-Mainandrina.michelPas encore d'évaluation
- 논문원문Document7 pages논문원문Donghee LeePas encore d'évaluation
- Diagnostics: Mobile Health in Remote Patient Monitoring For Chronic Diseases: Principles, Trends, and ChallengesDocument32 pagesDiagnostics: Mobile Health in Remote Patient Monitoring For Chronic Diseases: Principles, Trends, and ChallengesEngahmed IsmailPas encore d'évaluation
- Prevalence and Risk Factors For ChronicDocument10 pagesPrevalence and Risk Factors For ChronicKhoirul AnamPas encore d'évaluation
- Mhealth Interventions To Improve Cancer Screening and Early Detection: Scoping Review of ReviewsDocument19 pagesMhealth Interventions To Improve Cancer Screening and Early Detection: Scoping Review of ReviewsSiti MunawwarahPas encore d'évaluation
- Association Rules To Analyze Hospital Resources With Mortality RatesDocument7 pagesAssociation Rules To Analyze Hospital Resources With Mortality RatesIJRASETPublicationsPas encore d'évaluation
- Direct Costs of Parkinson's Disease in Brazil: A Case StudyDocument8 pagesDirect Costs of Parkinson's Disease in Brazil: A Case StudyIJAERS JOURNALPas encore d'évaluation
- Prevalence of Risk Factors of Non-Communicable Diseases in The Sultanate of Oman: STEPS Survey 2017Document23 pagesPrevalence of Risk Factors of Non-Communicable Diseases in The Sultanate of Oman: STEPS Survey 2017Muhrijal NurPas encore d'évaluation
- A Prospective Descriptive Study of Trauma Registry in Netaji Subhash Chandra Bose Medical College, JabalpurDocument9 pagesA Prospective Descriptive Study of Trauma Registry in Netaji Subhash Chandra Bose Medical College, JabalpurIJAR JOURNALPas encore d'évaluation
- Issm Prisma ChecklistDocument9 pagesIssm Prisma ChecklistInnani Wildania HusnaPas encore d'évaluation
- Prevalence of Diabetes in ArmyDocument12 pagesPrevalence of Diabetes in Armydhanusat20001828Pas encore d'évaluation
- Identification and Prediction of Chronic Diseases Using MachineDocument9 pagesIdentification and Prediction of Chronic Diseases Using MachineMuhammad Sadiq Khan NasarPas encore d'évaluation
- Paper 1Document13 pagesPaper 1Michael JamesPas encore d'évaluation
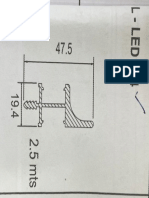
- Utturkar Wall L-Led 214 ProfileDocument1 pageUtturkar Wall L-Led 214 ProfileAngad SinghPas encore d'évaluation
- Shed DetailsDocument6 pagesShed DetailsAngad SinghPas encore d'évaluation
- 100 Beded Cancer HospitalDocument23 pages100 Beded Cancer Hospitalsureshvgk100% (1)
- Nursing Home 200 Beded PDFDocument40 pagesNursing Home 200 Beded PDFarun_tushar67% (3)
- 1business EnvironmentDocument13 pages1business EnvironmentAngad SinghPas encore d'évaluation
- Schedules of Shared Day Companies - MITCOEDocument1 pageSchedules of Shared Day Companies - MITCOEKalpak ShahanePas encore d'évaluation
- Family Code Cases Full TextDocument69 pagesFamily Code Cases Full TextNikki AndradePas encore d'évaluation
- PERDEV2Document7 pagesPERDEV2Riza Mae GardosePas encore d'évaluation
- 78 Complaint Annulment of Documents PDFDocument3 pages78 Complaint Annulment of Documents PDFjd fang-asanPas encore d'évaluation
- Modernity and Politics in IndiaDocument27 pagesModernity and Politics in Indiaarun_shivananda2754Pas encore d'évaluation
- StarbucksDocument19 pagesStarbucksPraveen KumarPas encore d'évaluation
- RPA Solutions - Step Into The FutureDocument13 pagesRPA Solutions - Step Into The FutureThe Poet Inside youPas encore d'évaluation
- Basic Fortigate Firewall Configuration: Content at A GlanceDocument17 pagesBasic Fortigate Firewall Configuration: Content at A GlanceDenisa PriftiPas encore d'évaluation
- Chapter 1 Basic-Concepts-Of-EconomicsDocument30 pagesChapter 1 Basic-Concepts-Of-EconomicsNAZMULPas encore d'évaluation
- Lec 15. National Income Accounting V3 REVISEDDocument33 pagesLec 15. National Income Accounting V3 REVISEDAbhijeet SinghPas encore d'évaluation
- Department of Planning and Community Development: Organizational ChartDocument5 pagesDepartment of Planning and Community Development: Organizational ChartkeithmontpvtPas encore d'évaluation
- Online Advertising BLUE BOOK: The Guide To Ad Networks & ExchangesDocument28 pagesOnline Advertising BLUE BOOK: The Guide To Ad Networks & ExchangesmThink100% (1)
- Swot MerckDocument3 pagesSwot Mercktomassetya0% (1)
- Three VignettesDocument3 pagesThree VignettesIsham IbrahimPas encore d'évaluation
- British Airways Vs CADocument17 pagesBritish Airways Vs CAGia DimayugaPas encore d'évaluation
- JAR66Document100 pagesJAR66Nae GabrielPas encore d'évaluation
- 2018-Gray-Life, Death, or Zombie - The Vitality of International OrganizationsDocument13 pages2018-Gray-Life, Death, or Zombie - The Vitality of International OrganizationsNightWalkerPas encore d'évaluation
- Tok SB Ibdip Ch1Document16 pagesTok SB Ibdip Ch1Luis Andrés Arce SalazarPas encore d'évaluation
- A Collection of Poems by AKDocument16 pagesA Collection of Poems by AKAnanda KrishnanPas encore d'évaluation
- List of Ielts Speking Part 3Document20 pagesList of Ielts Speking Part 3Kumiko LinoPas encore d'évaluation
- Special Power of Attorney: Know All Men by These PresentsDocument1 pageSpecial Power of Attorney: Know All Men by These PresentsTonie NietoPas encore d'évaluation
- Ppg-Gdch-Nur-45 Crash Cart Maintenance and ChecksDocument5 pagesPpg-Gdch-Nur-45 Crash Cart Maintenance and ChecksKenny JosefPas encore d'évaluation
- AKL - Pert 2-2Document2 pagesAKL - Pert 2-2Astri Ririn ErnawatiPas encore d'évaluation
- Project On Hospitality Industry: Customer Relationship ManagementDocument36 pagesProject On Hospitality Industry: Customer Relationship ManagementShraddha TiwariPas encore d'évaluation
- Greek Gods & Goddesses (Gods & Goddesses of Mythology) PDFDocument132 pagesGreek Gods & Goddesses (Gods & Goddesses of Mythology) PDFgie cadusalePas encore d'évaluation
- Ethiopia Pulp & Paper SC: Notice NoticeDocument1 pageEthiopia Pulp & Paper SC: Notice NoticeWedi FitwiPas encore d'évaluation
- Philippine CuisineDocument1 pagePhilippine CuisineEvanFerrerPas encore d'évaluation
- Digi Bill 13513651340.010360825015067633Document7 pagesDigi Bill 13513651340.010360825015067633DAVENDRAN A/L KALIAPPAN MoePas encore d'évaluation
- Monopolistic CompetitionDocument4 pagesMonopolistic CompetitionAzharPas encore d'évaluation
- WAS 101 EditedDocument132 pagesWAS 101 EditedJateni jotePas encore d'évaluation
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryD'EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryÉvaluation : 4.5 sur 5 étoiles4.5/5 (157)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisD'EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (9)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreD'EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreÉvaluation : 5 sur 5 étoiles5/5 (17)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesD'EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesÉvaluation : 5 sur 5 étoiles5/5 (70)
- An Autobiography of Trauma: A Healing JourneyD'EverandAn Autobiography of Trauma: A Healing JourneyÉvaluation : 5 sur 5 étoiles5/5 (2)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeD'EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeÉvaluation : 4.5 sur 5 étoiles4.5/5 (140)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDD'EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDÉvaluation : 4.5 sur 5 étoiles4.5/5 (167)
- Vagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerD'EverandVagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerÉvaluation : 4.5 sur 5 étoiles4.5/5 (16)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionD'EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionPas encore d'évaluation
- Triggers: How We Can Stop Reacting and Start HealingD'EverandTriggers: How We Can Stop Reacting and Start HealingÉvaluation : 5 sur 5 étoiles5/5 (58)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsD'EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsÉvaluation : 4.5 sur 5 étoiles4.5/5 (39)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeD'EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeÉvaluation : 4.5 sur 5 étoiles4.5/5 (49)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeD'EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeÉvaluation : 5 sur 5 étoiles5/5 (558)
- Brain Inflamed: Uncovering the Hidden Causes of Anxiety, Depression, and Other Mood Disorders in Adolescents and TeensD'EverandBrain Inflamed: Uncovering the Hidden Causes of Anxiety, Depression, and Other Mood Disorders in Adolescents and TeensÉvaluation : 5 sur 5 étoiles5/5 (2)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaD'EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (56)
- I Don't Want to Talk About It: Overcoming the Secret Legacy of Male DepressionD'EverandI Don't Want to Talk About It: Overcoming the Secret Legacy of Male DepressionÉvaluation : 4 sur 5 étoiles4/5 (74)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveD'EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveÉvaluation : 4 sur 5 étoiles4/5 (250)
- Don't Panic: Taking Control of Anxiety AttacksD'EverandDon't Panic: Taking Control of Anxiety AttacksÉvaluation : 4 sur 5 étoiles4/5 (12)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisD'EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisÉvaluation : 5 sur 5 étoiles5/5 (5)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIOND'EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONÉvaluation : 4.5 sur 5 étoiles4.5/5 (24)
- Embrace Your Weird: Face Your Fears and Unleash CreativityD'EverandEmbrace Your Weird: Face Your Fears and Unleash CreativityÉvaluation : 4.5 sur 5 étoiles4.5/5 (124)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsD'EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsÉvaluation : 4.5 sur 5 étoiles4.5/5 (48)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionD'EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionÉvaluation : 4 sur 5 étoiles4/5 (11)