Vous aimerez peut-être aussi
- Master the Boards: USMLE Step 2 CK UpdatesDocument4 pagesMaster the Boards: USMLE Step 2 CK Updatesultimate knowledgezonePas encore d'évaluation
- Week 9: Course Task-Case Analysis Renal DisordersDocument4 pagesWeek 9: Course Task-Case Analysis Renal DisordersBELTRAN, JEANNE MAURICEPas encore d'évaluation
- Right Side Pleuritic Chest Pain For A Few Hours. On Examination Tachycardia, Respiratory Distress, O Breath Sounds On The Right SideDocument9 pagesRight Side Pleuritic Chest Pain For A Few Hours. On Examination Tachycardia, Respiratory Distress, O Breath Sounds On The Right SideRabia RabiaPas encore d'évaluation
- AIIMS NORCET 2022 Memory Based Paper 11th September 2022 EnglishDocument20 pagesAIIMS NORCET 2022 Memory Based Paper 11th September 2022 EnglishMata BharatPas encore d'évaluation
- SCHS Nursing Specialist Exam Model 4Document8 pagesSCHS Nursing Specialist Exam Model 4Ahmad Khalil Al Sadi100% (7)
- OIIQ Prep QuestionsDocument10 pagesOIIQ Prep QuestionsDan Thanh Luu67% (3)
- Lekarski Egzamin Końcowy pytania z medycyny ratunkowej i intensywnej terapiiDocument74 pagesLekarski Egzamin Końcowy pytania z medycyny ratunkowej i intensywnej terapiiDev RishabPas encore d'évaluation
- Haad 1Document9 pagesHaad 1AcohCChaoPas encore d'évaluation
- Medsurge RationaleDocument8 pagesMedsurge RationaleRose Anne AbivaPas encore d'évaluation
- B - Mini and OSCEDocument7 pagesB - Mini and OSCEMohammad AlrefaiPas encore d'évaluation
- UntitledDocument7 pagesUntitledRabia RabiaPas encore d'évaluation
- Holistic Treatment of Lyme DiseaseDocument54 pagesHolistic Treatment of Lyme Diseasefrederic9866Pas encore d'évaluation
- MTB Errata CorrectionsDocument2 pagesMTB Errata CorrectionsAxel NunezPas encore d'évaluation
- NMC CBT MOCK TEST 4 REVIEWDocument13 pagesNMC CBT MOCK TEST 4 REVIEWCharles Osiako100% (1)
- Internal Medicine 1 Conrad FischerDocument35 pagesInternal Medicine 1 Conrad Fischerjaber fathiPas encore d'évaluation
- Febrile SeizuresDocument11 pagesFebrile SeizuresLita Al AmudiPas encore d'évaluation
- High Yield Step 2ckDocument4 pagesHigh Yield Step 2ckCesar_Palana_3832Pas encore d'évaluation
- Evaluation of In-Patients With FeverDocument125 pagesEvaluation of In-Patients With FeverStangPongritPas encore d'évaluation
- Leadership & Management PrioritizationDocument106 pagesLeadership & Management Prioritizationamasoud96 amasoud96Pas encore d'évaluation
- Medicine and Surgery Review QuestionsDocument5 pagesMedicine and Surgery Review QuestionsLamya BanderPas encore d'évaluation
- Mock CodeDocument4 pagesMock CodeKrezielDulosEscobarPas encore d'évaluation
- Emergency Response to AnaphylaxisDocument9 pagesEmergency Response to AnaphylaxisAlqi YuthaPas encore d'évaluation
- Concept MapDocument1 pageConcept Mapapi-246466200Pas encore d'évaluation
- Pediatrics MS WordDocument13 pagesPediatrics MS WordSamhitha SharmaPas encore d'évaluation
- Listening OET 2.0 LDocument177 pagesListening OET 2.0 Lgyby_nairPas encore d'évaluation
- HAAD Q and ADocument100 pagesHAAD Q and Aleah100% (24)
- лекц10Document41 pagesлекц10A A D H IPas encore d'évaluation
- Causes, treatments, diagnoses and management of common medical conditionsDocument15 pagesCauses, treatments, diagnoses and management of common medical conditionsnada elfarraPas encore d'évaluation
- MCCEE2003May PDFDocument19 pagesMCCEE2003May PDFdimdamflyPas encore d'évaluation
- Task Full TopicsDocument36 pagesTask Full TopicsReshma Shaji PnsPas encore d'évaluation
- Quiz Critical CareDocument15 pagesQuiz Critical CareSuma AhmadPas encore d'évaluation
- Common bacteria in calf diarrhoeaDocument8 pagesCommon bacteria in calf diarrhoeaBorja Bueno GarciaPas encore d'évaluation
- Caudal S(+)-ketamine prolongs postoperative analgesia vs IV in pediatric surgeryDocument35 pagesCaudal S(+)-ketamine prolongs postoperative analgesia vs IV in pediatric surgerynabilchyPas encore d'évaluation
- Neuro - ICPDocument24 pagesNeuro - ICPcsePas encore d'évaluation
- NCLEX Tips for SuccessDocument8 pagesNCLEX Tips for SuccessManuel Láncara100% (1)
- MRCP 2016 September 1Document32 pagesMRCP 2016 September 1Abdullah Mohammad Ibne HaiderPas encore d'évaluation
- This Is A Single-Answer Multiple-Choice Examination. There Is Only One Correct Answer To Each QuestionDocument8 pagesThis Is A Single-Answer Multiple-Choice Examination. There Is Only One Correct Answer To Each QuestionUgeshwaran Aristotle Reddy50% (2)
- Diagnosis and Management Medical ScenariosDocument12 pagesDiagnosis and Management Medical Scenariosnreena aslam100% (3)
- Free 120 March 2021 Explanation 2Document62 pagesFree 120 March 2021 Explanation 2Enrique ParedesPas encore d'évaluation
- Emergency MedicineDocument46 pagesEmergency MedicinekararobeedPas encore d'évaluation
- Analisis Jurnal Electric Blanket and Forced AirDocument12 pagesAnalisis Jurnal Electric Blanket and Forced AirWedaswari WidyaPas encore d'évaluation
- 2 EclampsiaDocument17 pages2 EclampsiaDrMohammad KhadrawyPas encore d'évaluation
- SCHS Nursing Specialist Exam Model 5Document8 pagesSCHS Nursing Specialist Exam Model 5Ahmad Khalil Al Sadi100% (2)
- Acute Cardiac CareDocument42 pagesAcute Cardiac CareMarwa Elsayed Abuelnour100% (1)
- Course Task CU2Document3 pagesCourse Task CU2Camille MactalPas encore d'évaluation
- Jurnal Jeliya TRSLTDocument10 pagesJurnal Jeliya TRSLTflosimarmataPas encore d'évaluation
- General Surgery MCQDocument190 pagesGeneral Surgery MCQلمسة مصمم100% (1)
- Usmle 2ck Practice Questions All 2015Document6 pagesUsmle 2ck Practice Questions All 2015Sharmela BrijmohanPas encore d'évaluation
- Anafilaxic ReactionsDocument9 pagesAnafilaxic ReactionsAlqi YuthaPas encore d'évaluation
- General Surgery MCQDocument249 pagesGeneral Surgery MCQShriyansh Chahar88% (8)
- Osce PuneDocument75 pagesOsce PuneGhada ElhassanPas encore d'évaluation
- Learning Station 2 Electrolyte Abnormalities: ©1999 American Heart AssociationDocument57 pagesLearning Station 2 Electrolyte Abnormalities: ©1999 American Heart AssociationbrentupdegraffPas encore d'évaluation
- Nclex Notes 1Document17 pagesNclex Notes 1itokumo100% (2)
- Auto Digestion of The PancreasDocument13 pagesAuto Digestion of The PancreasJincy JosePas encore d'évaluation
- 1-Done-Key Medicine A-Supply 2021Document6 pages1-Done-Key Medicine A-Supply 2021Rabia RabiaPas encore d'évaluation
- Recall ADocument86 pagesRecall ANikhil WaliaPas encore d'évaluation
- Mastery Question MDFDocument66 pagesMastery Question MDFshaaish100% (1)
- Materi MCQDocument15 pagesMateri MCQRaqqi PujatmikoPas encore d'évaluation
- Basic Skills in NursingDocument82 pagesBasic Skills in NursingMichael SedanoPas encore d'évaluation
- 562ue 2014-06Document55 pages562ue 2014-06vijayramaswamyPas encore d'évaluation
- Academic Writing in English: Carolyn Brimley Norris, Ph.D. Language Services University of Helsinki 2015Document86 pagesAcademic Writing in English: Carolyn Brimley Norris, Ph.D. Language Services University of Helsinki 2015nasralaPas encore d'évaluation
- Sample OMR Sheet Marking PDFDocument1 pageSample OMR Sheet Marking PDFMuraliPas encore d'évaluation
- Module 6 - Arabic LiteratureDocument26 pagesModule 6 - Arabic LiteratureFrancis TatelPas encore d'évaluation
- Surviving A Zombie ApocalypseDocument4 pagesSurviving A Zombie ApocalypseSarah SmithPas encore d'évaluation
- Ponnu ThomasDocument155 pagesPonnu ThomasWinston KennethPas encore d'évaluation
- BengzonDocument5 pagesBengzonmceline19Pas encore d'évaluation
- Public Service Commission, West Bengal: Notice Inviting Expression of Interest For Enlistment As LawyersDocument3 pagesPublic Service Commission, West Bengal: Notice Inviting Expression of Interest For Enlistment As LawyersITI JobPas encore d'évaluation
- Investigation Into Failure Phenomena of Water Meter in The Kingdom of BahrainDocument118 pagesInvestigation Into Failure Phenomena of Water Meter in The Kingdom of BahrainJabnon NonjabPas encore d'évaluation
- Pamela Presentation PDFDocument8 pagesPamela Presentation PDFawtshfhdPas encore d'évaluation
- AnalogyDocument50 pagesAnalogyNathaniel Campeciño89% (9)
- MICEDocument37 pagesMICECeleste Torino DigalPas encore d'évaluation
- FORMS Transaction DisputeDocument1 pageFORMS Transaction DisputeKristine Cruz-MaltoPas encore d'évaluation
- Kerala University of Health Sciences Faculty of Dentistry BDS Course Regulations and Syllabus 2010Document125 pagesKerala University of Health Sciences Faculty of Dentistry BDS Course Regulations and Syllabus 2010Shyam KrishnanPas encore d'évaluation
- Guía BaccettiDocument11 pagesGuía BaccettiPercy Andree Bayona GuillermoPas encore d'évaluation
- Pityriasis Versicolor: Avoiding Pitfalls in Disease Diagnosis and TherapyDocument3 pagesPityriasis Versicolor: Avoiding Pitfalls in Disease Diagnosis and TherapypanduPas encore d'évaluation
- Charatible Trust FINAL BOOKDocument80 pagesCharatible Trust FINAL BOOKAmitPas encore d'évaluation
- BS en 01062-3-2008 PDFDocument12 pagesBS en 01062-3-2008 PDFjohnPas encore d'évaluation
- 2016 UCF Depth ChartDocument1 page2016 UCF Depth ChartBrandon HelwigPas encore d'évaluation
- Transits of The Year 2008: Text by Robert HandDocument27 pagesTransits of The Year 2008: Text by Robert HandjasminnexPas encore d'évaluation
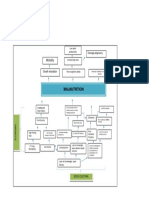
- Problem Tree Analysis MalnutritionDocument1 pageProblem Tree Analysis MalnutritionMho Dsb50% (6)
- Complete Dermatology NotesDocument41 pagesComplete Dermatology NotesSetlhare MotsamaiPas encore d'évaluation
- Left Movement in India Before IndependenceDocument3 pagesLeft Movement in India Before IndependenceMahesh KumarPas encore d'évaluation
- The CatDocument2 pagesThe CatDodi SaputraPas encore d'évaluation
- Dwnload Full Principles of Foundation Engineering Si Edition 7th Edition Das Solutions Manual PDFDocument36 pagesDwnload Full Principles of Foundation Engineering Si Edition 7th Edition Das Solutions Manual PDFwelked.gourami8nu9d100% (10)
- SAP Two-Phase CommitDocument39 pagesSAP Two-Phase CommitSudhanshu DuttaPas encore d'évaluation
- Karma Connection in Marriage PDFDocument27 pagesKarma Connection in Marriage PDFAavesh TapdePas encore d'évaluation
- Civ Pro I - 2011 TahaDocument27 pagesCiv Pro I - 2011 TahaACDCPas encore d'évaluation
- Dr. Kirti MatliwalaDocument6 pagesDr. Kirti MatliwalaKirti Dakshesh ThakarPas encore d'évaluation