Vous aimerez peut-être aussi
- SpirometriDocument1 pageSpirometriAri Julian SaputraPas encore d'évaluation
- Effect of Stay Up All NightDocument11 pagesEffect of Stay Up All NightAri Julian SaputraPas encore d'évaluation
- Nervus Laryngeus RecurrensDocument5 pagesNervus Laryngeus RecurrensAri Julian SaputraPas encore d'évaluation
- Sepsis Neonatorum PDFDocument2 pagesSepsis Neonatorum PDFAri Julian SaputraPas encore d'évaluation
- DapussDocument1 pageDapussAri Julian SaputraPas encore d'évaluation
- Anatomy of Plexus BranchialisDocument24 pagesAnatomy of Plexus BranchialisAri Julian SaputraPas encore d'évaluation
- Diagnosing TB Infection in Children: Analysis of Discordances Using in Vitro Tests and The Tuberculin Skin TestDocument9 pagesDiagnosing TB Infection in Children: Analysis of Discordances Using in Vitro Tests and The Tuberculin Skin TestAri Julian SaputraPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Energies: Numerical Simulations On The Application of A Closed-Loop Lake Water Heat Pump System in The Lake Soyang, KoreaDocument16 pagesEnergies: Numerical Simulations On The Application of A Closed-Loop Lake Water Heat Pump System in The Lake Soyang, KoreaMvikeli DlaminiPas encore d'évaluation
- File3 PDFDocument119 pagesFile3 PDFikkemijnnaam0% (1)
- Quarter 2 Week 5Document54 pagesQuarter 2 Week 5rixzylicoqui.salcedoPas encore d'évaluation
- PCB Engraver Operator Manual PDFDocument41 pagesPCB Engraver Operator Manual PDFmyoshkeuPas encore d'évaluation
- Random FactsDocument353 pagesRandom FactsSergio Rivas100% (1)
- 6th Grade Spelling ListsDocument10 pages6th Grade Spelling Listsapi-326416336Pas encore d'évaluation
- Hernandez Vs CADocument1 pageHernandez Vs CAAnonymous WXk7CCRI9LPas encore d'évaluation
- LIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyDocument2 pagesLIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyBenjamin TantiansuPas encore d'évaluation
- Amp. 100 Watt ExtractedDocument6 pagesAmp. 100 Watt ExtractedJosue CórdovaPas encore d'évaluation
- VSR 411 QB AnaesthesiaDocument7 pagesVSR 411 QB Anaesthesiavishnu dathPas encore d'évaluation
- Application of Knowledge QuestionsDocument16 pagesApplication of Knowledge QuestionsElllie TattersPas encore d'évaluation
- Lesson 1 Animal CareDocument8 pagesLesson 1 Animal CareLexi PetersonPas encore d'évaluation
- EV-H-A1R 54C - M - EN - 2014 - D - Heat Detector SalwicoDocument2 pagesEV-H-A1R 54C - M - EN - 2014 - D - Heat Detector SalwicoCarolinaPas encore d'évaluation
- Afico Pipe InsulaionDocument4 pagesAfico Pipe InsulaionProcurement AlamcoPas encore d'évaluation
- NACH FormDocument2 pagesNACH FormShreyas WaghmarePas encore d'évaluation
- Assignment 2 ME 326Document10 pagesAssignment 2 ME 326divided.symphonyPas encore d'évaluation
- (PDF) Books Toxic Parents Epub Popular Download - by Susan ForwardDocument1 page(PDF) Books Toxic Parents Epub Popular Download - by Susan Forwardmartagonzalezbordonaba0% (3)
- AD Oracle ManualDocument18 pagesAD Oracle ManualAlexandru Octavian Popîrțac100% (2)
- Management of AsthmaDocument29 pagesManagement of AsthmaAbdullah Al ArifPas encore d'évaluation
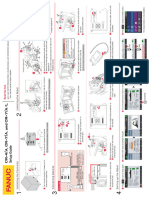
- CR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)Document1 pageCR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)lidiia.pavlkukPas encore d'évaluation
- Barangay Clearance SampleDocument1 pageBarangay Clearance SampleBarangay Onse Malaybalay100% (3)
- 621F 721F Op's ManualDocument362 pages621F 721F Op's ManualMilAuto87100% (1)
- Jis C 8156-2017, EngDocument32 pagesJis C 8156-2017, Eng7620383tlPas encore d'évaluation
- Coatings and Waterproofing: KhalafDocument19 pagesCoatings and Waterproofing: KhalafmohamedPas encore d'évaluation
- Nepal Health Research CouncilDocument15 pagesNepal Health Research Councilnabin hamalPas encore d'évaluation
- Questions To Client On SAP HCMDocument19 pagesQuestions To Client On SAP HCMeurofighterPas encore d'évaluation
- Evolution of Fluidized Bed TechnologyDocument17 pagesEvolution of Fluidized Bed Technologyika yuliyani murtiharjonoPas encore d'évaluation
- Applying Sarf Book 1 - Published-46-59Document14 pagesApplying Sarf Book 1 - Published-46-59Nauman AbbasPas encore d'évaluation
- All About 304 Steel (Properties, Strength, and Uses)Document7 pagesAll About 304 Steel (Properties, Strength, and Uses)ZebPas encore d'évaluation
- Heating System Design (Student)Document25 pagesHeating System Design (Student)markbrennan1Pas encore d'évaluation