Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Sexual Self: Presented By: Group 1Document26 pagesSexual Self: Presented By: Group 1Vanessa Joyce Isleta100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Prostate Massage - Wikipedia, The Free EncyclopediaDocument5 pagesProstate Massage - Wikipedia, The Free EncyclopediaA R KhanPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- How To Position Finerenone in The Treatment Algorithm For Type 2 Diabetes With Renal Complication - GPMPDocument27 pagesHow To Position Finerenone in The Treatment Algorithm For Type 2 Diabetes With Renal Complication - GPMPTaufiqurrokhman RofiiPas encore d'évaluation
- Male Reproductive Anatomy and Physiology: 1. PenisDocument7 pagesMale Reproductive Anatomy and Physiology: 1. PenisMhiahLine TolentinoPas encore d'évaluation
- Glomerulonephritis: Lecturer Prof. Yu.R. KovalevDocument39 pagesGlomerulonephritis: Lecturer Prof. Yu.R. Kovalevalfaz lakhani100% (1)
- F.calise, L.casciola - Minimally Invasive Surgery of The Liver - 2013Document320 pagesF.calise, L.casciola - Minimally Invasive Surgery of The Liver - 2013Cotaga IgorPas encore d'évaluation
- b9 PKM 2 Urinary Retention Dr. Christian Ronald Tanggo Sp.uDocument63 pagesb9 PKM 2 Urinary Retention Dr. Christian Ronald Tanggo Sp.uDaud ParluhutanPas encore d'évaluation
- Instructions For Completing The 3-Day Voiding DiaryDocument4 pagesInstructions For Completing The 3-Day Voiding DiaryAgil SaputraPas encore d'évaluation
- Thomson - The Excretory SystemDocument24 pagesThomson - The Excretory Systemapi-263178717Pas encore d'évaluation
- Kidney F Post TestDocument4 pagesKidney F Post TestMardie ArcesPas encore d'évaluation
- UTI, HSC With QuestionsDocument43 pagesUTI, HSC With QuestionsAlex MatthewPas encore d'évaluation
- Thesis Topics On Urinary Tract InfectionDocument7 pagesThesis Topics On Urinary Tract Infectionsusantullisnorman100% (2)
- STD Risk Assessment QuestionnaireDocument1 pageSTD Risk Assessment QuestionnaireTine GuibaoPas encore d'évaluation
- Corn SilkDocument1 pageCorn Silkwillyagung4557Pas encore d'évaluation
- Acute Renal Failure-Step23C - 1Document28 pagesAcute Renal Failure-Step23C - 1DEBJIT SARKARPas encore d'évaluation
- Case Draft BPHDocument20 pagesCase Draft BPHKceey CruzPas encore d'évaluation
- 21 y/o male with dysuria and UTI diagnosed with E. coli, N. gonorrheaDocument2 pages21 y/o male with dysuria and UTI diagnosed with E. coli, N. gonorrheaGerald John PazPas encore d'évaluation
- Piuria EsterilDocument4 pagesPiuria EsterilBruno Vilela MonteiroPas encore d'évaluation
- Benign Prostatic Hyperplasia Is A BenignDocument4 pagesBenign Prostatic Hyperplasia Is A BenignZeinab SrourPas encore d'évaluation
- Urethritis, STD, Mycoplasma or Chlamydia InfectionDocument11 pagesUrethritis, STD, Mycoplasma or Chlamydia InfectionbetebetPas encore d'évaluation
- Aafp Uti GuidelinesDocument10 pagesAafp Uti GuidelinesCess Lagera YbanezPas encore d'évaluation
- Kontraindikasi CircumsisiDocument23 pagesKontraindikasi CircumsisiElfi MuazzamPas encore d'évaluation
- Intermittent Catheterization and LoFricDocument32 pagesIntermittent Catheterization and LoFricmokilpoPas encore d'évaluation
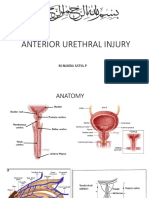
- Rupture Urethra Anterior DR Sule FixDocument36 pagesRupture Urethra Anterior DR Sule FixkadinfathiaPas encore d'évaluation
- UrinDocument2 pagesUrinnacha nurhasanahPas encore d'évaluation
- BPH Treatment and Surgical OptionsDocument25 pagesBPH Treatment and Surgical OptionsShreevidya GurunageshPas encore d'évaluation
- Unite 6Document17 pagesUnite 6Surafel TamratPas encore d'évaluation
- Urine Full Exam and Microscopic Exam (UrinalysisDocument11 pagesUrine Full Exam and Microscopic Exam (UrinalysisKarthigaRamanPas encore d'évaluation
- P7 TR Apg 2020Document26 pagesP7 TR Apg 2020Lia NurPas encore d'évaluation
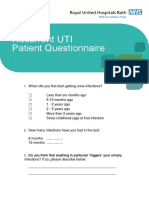
- UTI Pathway Patient QuestionnaireDocument4 pagesUTI Pathway Patient QuestionnaireRuby Liza CapatePas encore d'évaluation